Download
1 / 1
20 likes | 179 Views
In Utero NHP Imaging and monkey fetus imaging. Carlos A. Castro 2 , Parker H. Mills 1 , John A. Ozolek 2 , Eric T. Ahrens 1 , Gerald P. Schatten 2 1 Department of Biological Sciences and the Pittsburgh NMR Center for Biomedical Research, Carnegie Mellon University, Pittsburgh, PA,

E N D
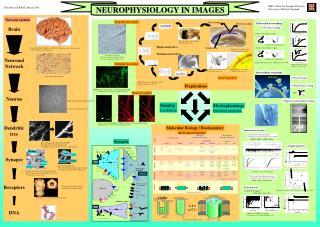
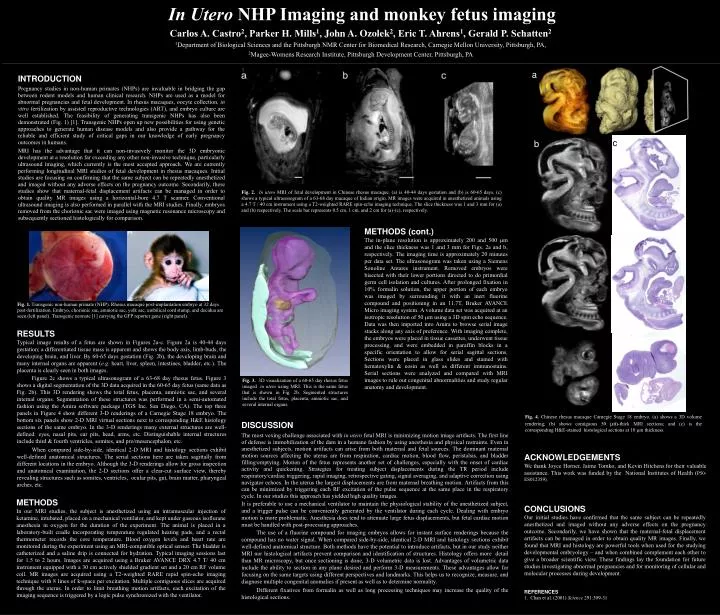
In Utero NHP Imaging and monkey fetus imaging Carlos A. Castro2, Parker H. Mills1, John A. Ozolek2, Eric T. Ahrens1, Gerald P. Schatten2 1Department of Biological Sciences and the Pittsburgh NMR Center for Biomedical Research, Carnegie Mellon University, Pittsburgh, PA, 2Magee-Womens Research Institute, Pittsburgh Development Center, Pittsburgh, PA a INTRODUCTION Pregnancy studies in non-human primates (NHPs) are invaluable in bridging the gap between rodent models and human clinical research. NHPs are used as a model for abnormal pregnancies and fetal development. In rhesus macaques, oocyte collection, in vitro fertilization by assisted reproductive technologies (ART), and embryo culture are well established. The feasibility of generating transgenic NHPs has also been demonstrated (Fig. 1) [1]. Transgenic NHPs open up new possibilities for using genetic approaches to generate human disease models and also provide a pathway for the reliable and efficient study of critical gaps in our knowledge of early pregnancy outcomes in humans. MRI has the advantage that it can non-invasively monitor the 3D embryonic development at a resolution far exceeding any other non-invasive technique, particularly ultrasound imaging, which currently is the most accepted approach. We are currently performing longitudinal MRI studies of fetal development in rhesus macaques. Initial studies are focusing on confirming that the same subject can be repeatedly anesthetized and imaged without any adverse effects on the pregnancy outcome. Secondarily, these studies show that maternal-fetal displacement artifacts can be managed in order to obtain quality MR images using a horizontal-bore 4.7 T scanner. Conventional ultrasound imaging is also performed in parallel with the MRI studies. Finally, embryos removed from the chorionic sac were imaged using magnetic resonance microscopy and subsequently sectioned histologically for comparison. c b Fig. 2. In utero MRI of fetal development in Chinese rhesus macaque. (a) is 40-44 days gestation and (b) is 60-65 days. (c) shows a typical ultrasonogram of a 63-68 day macaque of Indian origin. MR images were acquired in anesthetized animals using a 4.7 T / 40 cm instrument using a T2-weighted RARE spin-echo imaging technique. The slice thickness was 1 and 3 mm for (a) and (b) respectively. The scale bar represents 0.5 cm, 1 cm, and 2 cm for (a)-(c), respectively. METHODS (cont.) The in-plane resolution is approximately 200 and 500 mm and the slice thickness was 1 and 3 mmfor Figs. 2a and b, respectively. The imaging time is approximately 20 minutes per data set. The ultrasonogram was taken using a Siemens Sonoline Antares instrument. Removed embryos were bisected with their lower portions directed to do primordial germ cell isolation and cultures. After prolonged fixation in 10% formalin solution, the upper portion of each embryo was imaged by surrounding it with an inert fluorine compound and positioning in an 11.7T, Bruker AVANCE Micro imaging system. A volume data set was acquired at an isotropic resolution of 50 mm using a 3D spin echo sequence. Data was then imported into Amira to browse serial image stacks along any axis of preference. With imaging complete, the embryos were placed in tissue cassettes, underwent tissue processing, and were embedded in paraffin blocks in a specific orientation to allow for serial sagittal sections. Sections were placed in glass slides and stained with hematoxylin & eosin as well as different immunostains. Serial sections were analyzed and compared with MRI images to rule out congenital abnormalities and study regular anatomy and development. Fig. 1. Transgenic non-human primate (NHP). Rhesus macaque post-implantation embryo at 32 days post-fertilization. Embryo, chorionic sac, amniotic sac, yolk sac, umbilical cord stump, and decidua are seen.(left panel). Transgenic neonate [1] carrying the GFP reporter gene (right panel). RESULTS Typical image results of a fetus are shown in Figures 2a-c. Figure 2a is 40-44 days gestation; a differentiated tissue mass is apparent and shows the body axis, limb-buds, the developing brain, and liver. By 60-65 days gestation (Fig. 2b), the developing brain and many internal organs are apparent (e.g. heart, liver, spleen, intestines, bladder, etc.). The placenta is clearly seen in both images. Figure 2c shows a typical ultrasonogram of a 63-68 day rhesus fetus. Figure 3 shows a digital segmentation of the 3D data acquired in the 60-65 day fetus (same data as Fig. 2b). This 3D rendering shows the total fetus, placenta, amniotic sac, and several internal organs. Segmentation of these structures was performed in a semi-automated fashion using the Amira software package (TGS Inc. San Diego, CA). The top three panels in Figure 4 show different 3-D renderings of a Carnegie Stage 18 embryo. The bottom six panels show 2-D MRI virtual sections next to corresponding H&E histology sections of the same embryo. In the 3-D renderings many external structures are well-defined: eyes, nasal pits, ear pits, head, arms, etc. Distinguishable internal structures include third & fourth ventricles, somites, and pro/mesencephalon, etc. When compared side-by-side, identical 2-D MRI and histology sections exhibit well-defined anatomical structures. The serial sections here are taken sagittally from different locations in the embryo. Although the 3-D renderings allow for gross inspection and anatomical examination, the 2-D sections offer a clear-cut surface view, thereby revealing structures such as somites, ventricles, ocular pits, gut, brain matter, pharyngeal arches, etc. Fig. 3. 3D visualization of a 60-65 day rhesus fetus imaged in utero using MRI. This is the same fetus that is shown in Fig. 2b. Segmented structures include the total fetus, placenta, amniotic sac, and several internal organs. Fig. 4. Chinese rhesus macaque Carnegie Stage 18 embryo. (a) shows a 3D volume rendering; (b) shows contiguous 50 mm-thick MRI sections; and (c) is the corresponding H&E-stained histological sections at 10 mm thickness. DISCUSSION The most vexing challenge associated with in utero fetal MRI is minimizing motion image artifacts. The first line of defense is immobilization of the dam in a humane fashion by using anesthesia and physical restraints. Even in anesthetized subjects, motion artifacts can arise from both maternal and fetal sources. The dominant maternal motion sources affecting the uterus are from respiration, cardiac motion, blood flow, peristalsis, and bladder filling/emptying. Motion of the fetus represents another set of challenges, especially with the onset of cardiac activity and quickening. Strategies for treating subject displacements during the TR period include respiratory/cardiac triggering, rapid imaging, retrospective gating, signal averaging, and adaptive correction using navigator echoes. In the uterus the largest displacements are from maternal breathing motion. Artifacts from this can be minimized by triggering each RF excitation of the pulse sequence at the same place in the respiratory cycle. In our studies this approach has yielded high quality images. It is preferable to use a mechanical ventilator to maintain the physiological stability of the anesthetized subject, and a trigger pulse can be conveniently generated by the ventilator during each cycle. Dealing with embryo motion is more problematic. Anesthesia does tend to attenuate large fetus displacements, but fetal cardiac motion must be handled with post-processing approaches. The use of a fluorine compound for imaging embryos allows for instant surface renderings because the compound has no water signal. When compared side-by-side, identical 2-D MRI and histology sections exhibit well-defined anatomical structure. Both methods have the potential to introduce artifacts, but in our study neither MRI nor histological artifacts prevent comparison and identification of structures. Histology offers more detail than MR microscopy, but once sectioning is done, 3-D volumetric data is lost. Advantages of volumetric data include the ability to section in any plane desired and perform 3-D measurements. These advantages allow for focusing on the same targets using different perspectives and landmarks.This helps us to recognize, measure, and diagnose multiple congenital anomalies if present as well as to determine normality. Different fixatives from formalin as well as long processing techniques may increase the quality of the histological sections. Image number Image number ACKNOWLEDGEMENTS We thank Joyce Horner, Jaime Tomko, and Kevin Hitchensfor their valuable assistance. This work was funded by the National Institutes of Health (P50-ES012359). METHODS In our MRI studies, the subject is anesthetized using an intramuscular injection of ketamine, intubated, placed on a mechanical ventilator, and kept under gaseous isoflurane anesthesia in oxygen for the duration of the experiment. The animal is placed in a laboratory-built cradle incorporating temperature regulated heating pads, and a rectal thermometer records the core temperature. Blood oxygen levels and heart rate are monitored during the experiment using an MRI-compatible optical sensor. The bladder is catheterized and a saline drip is connected for hydration. Typical imaging sessions last for 1.5 to 2 hours. Images are acquired using a Bruker AVANCE DRX 4.7 T/ 40 cm instrument equipped with a 30 cm actively shielded gradient set and a 20 cm RF volume coil. MR images are acquired using a T2-weighted RARE rapid spin-echo imaging technique with 8 lines of k-space per excitation. Multiple contiguous slices are acquired through the uterus. In order to limit breathing motion artifacts, each excitation of the imaging sequence is triggered by a logic pulse synchronized with the ventilator. CONCLUSIONS Our initial studies have confirmed that the same subject can be repeatedly anesthetized and imaged without any adverse effects on the pregnancy outcome. Secondarily, we have shown that the maternal-fetal displacement artifacts can be managed in order to obtain quality MR images. Finally, we found that MRI and histology are powerful tools when used for the studying developmental embryology – and when combined complement each other to give a broader scientific view. These findings lay the foundation for future studies investigating abnormal pregnancies and for monitoring of cellular and molecular processes during development. REFERENCES 1. Chan et al. (2001) Science 291:309-31 Image number