Download

1 / 79
810 likes | 1.31k Views
Measuring Depth of Anesthesia. The word "anesthesia" was first used by the Greek philosopher Dioscorides in the first century of the current era to describe the narcotic effect of the plant mandragora.

E N D
The word "anesthesia" was first used by the Greek philosopher Dioscorides in the first century of the current era to describe the narcotic effect of the plant mandragora. • The word reappeared in the 1771 Encyclopaedia Britannica, where it was defined as a "privation of the senses.
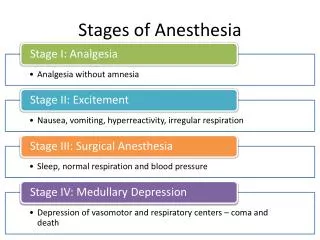
Plomley, in 1847, was the first to attempt to define depth of anesthesia. He described three stages: intoxication, excitement (both conscious and unconscious), and the deeper levels of narcosis. • In that same year, John Snow described "five degrees of narcotism" for ether anesthesia.
In 1937, Guedel published his classic description of the clinical signs of ether anesthesia. He used clear physical signs involving somatic muscle tone, respiratory patterns, and ocular signs to define four stages.
What Is Anesthesia? • The sine qua non of the anesthetized state is unconsciousness, the lack of conscious processing of thoughts. • The crux of the difficulty in defining anesthetic depth is that unconsciousness cannot be measured directly.
The most important is that for any stimulus response pair, depth of anesthesia is the probability of nonresponse. • More generally, depth of anesthesia is the probability of nonresponse to stimulation, calibrated against the strength of the stimulus, the diffiCulty of suppressing the response, and the drug-induced probability of nonresponsiveness.
Anesthetic depth ranges from a 100% probability of an easily suppressed response (verbal answer) to a mild stimulus (e.g., calling one's name) and readily suppressed responses (e.g., verbal answer) to a 100%probability of nonresponse to profoundly noxious stimuli (e.g., intubation) and responses that are difficult to suppress (e.g.,tachycardia).
response surfaces for a profoundstimulus movement response to intubation,
MEMORY AND AWARENESS • Recall, Conscious or Explicit Memory • Detection of Auditory Input, Unconscious or Implicit Memory
Recall, Conscious or Explicit Memory • Ghoneim recently reviewed cases of recall in different anesthetic situations. • The incidence of awareness in a non obstetric and noncardiac surgical population approximates 0.2%. • A higher incidence is reported for obstetric general anesthesia, 0.4%. • The incidence in cardiac surgery ranges from 1.1%to 1.5%. • major trauma cases can have a range of awareness from 11% to 43%.
Intraoperative awareness or recall has occurred with high-dose opioid anesthesia. • Two clinical signs possibly predicting the occurrence of recall are movement and autonomic response. • The use of muscle relaxants can eliminate the movement response, which leaves only autonomic activity as a measure of intraoperative awareness.
Detection of Auditory Input, Unconscious or Implicit Memory • Although the patient may not overtly recall a stimulus or an event, auditory input can register in the brain during apparently adequate surgical anesthesia. • Auditory and verbal input must be "meaningful" for it to register in the patient's memory. • Frequently, hypnosis or other cues may be needed to elicit recall.
Ten volunteers undergoing dental surgery were given thiopental followed by nitrous oxide and diethyl ether. Monitoring the EEG for an irregular slow-wave-high-voltage pattern allowed the anesthetist to maintain a similar depth of anesthesia in all patients. This EEGpattern was considered equivalent to moderate to deep ether anesthesia.
During surgery, the anesthetist provided verbal stimulation to the patient in the form of an intraoperative crisis by verbally stating that cyanosis was present and then treated appropriately.
All 10 patients had no spontaneous recall of the simulated intraoperative crisis. • Under hypnosis, however,four patients could remember the frightening words in exact detail. • An additional four remembered someone speaking to them. • All eight became anxious and either emerged spontaneously from their hypnotic trance or refused to continue exploring the event. • One subject had activation of the EEGpattern when the intraoperative crisis occurred, but no recall of the event.
Large effects on memory were produced only by propofol and midazolam. • Thiopental had mild memory effects, • whereas fentanyl had none.
Implications of Explicit, Intraoperative • Blacher described a traumatic post-cardiac surgery neurosis involving anxiety and irritability, repeated nightmares, preoccupation with death, and a reluctance to discuss these symptoms. • He attributed this postoperative state to patients' being awake and paralyzed during open heart surgery.
Inhaled Anesthetics • Movement Response and the MAC Concept: • MAC is the minimum alveolar concentration of inhaled anesthetic required to prevent 50% of subjects from responding to a painful stimulus with "gross purposeful movement.“ • For determination of MAC in humans, the standard noxious stimulus has been the initial surgical skin incision.
The MAC concept has been expanded by evaluating other clinical end points and defined stimuli. • the MAC of anesthetic that would allow opening of the eyes on verbal command during emergence from anesthesia ("MACawake) • Generally, MACawake values are a third to a fourth the MAC values for surgical incision.
the MAC of inhaled anesthetic that would inhibit movement and coughing during endotracheal intubation ("MACintubation"). • Intubation is significantly more stimulating than skin incision, and higher concentrations of inhaled anesthetic are required to eliminate the movement response.
MACBAR: The MAC of anesthetic necessary to prevent an adrenergic response to skin incision,as measured by the concentration of catecholamine in venous blood.
Because cerebral blood perfusion is large, it is possible to achieve an equilibration among end-tidal, alveolar, arterial, and brain anesthetic partial pressures within 15 minutes of exposure to a constant end-tidal anesthetic concentration. • If the difference between the inspired and end-tidal partial pressures was less than 10% difference between end-tidal and arterial concentrations would be minimal.
Eger and associates proposed that volatile anesthetics cause a lack of movement response to noxious stimuli by action in the spinal cord and create a hypnotic/amnestic loss of consciousness at a supraspinal, cortical site of action.
Other Clinical Responses: • Other Clinical Responses Responses other than purposeful movement have been investigated as possible clinical measures of the depth of anesthesia: • the rate and volume of ventilation in spontaneously breathing subjects, • eye movement, • the diameter and reactivity of pupils to light, • heart rate, • arterialblood pressure, • and autonomic signs such as sweating.
It has not been possible, however, to use these clinical signs to generate uniform measures of depth of anesthesia for inhaled anesthetics. Although some clinical signs do correlate with depth of anesthesia for certain inhaled anesthetics, the same cannot be said for other inhaled anesthetics.
Zbinden and colleagues systematically examined the interaction of isoflurane concentrations with the hemodynamic response to different noxious stimuli.
. When used as a sole agent, even at high concentrations isoflurane is unable to suppress hemodynamic responses to noxious stimuli. the addition of analgesic components, such as nitrous oxide and fentanyl, can prevent the sympathetic stimulation and hemodynamic responses seen with noxious surgical stimuli when inhaled anesthetics are used.
Intravenously Administered (Nonopioid)Anesthetics • Assessing Depth during Induction of Anesthesia • Assessing Depth during Maintenance of Anesthes
Assessing Depth during Induction of Anesthesia Induction of anesthesia often consists of a rapid intravenous bolus injection of a hypnotic (e.g., propofol,thiopental, etomidate). Plasma concentrations peak within a half to 1 minute and decline rapidly on redistribution of the drug.
Clinical end points useful in assessing the depth of anesthesia during induction include loss of verbal responsiveness, loss of eyelid reflex, and loss of corneal reflex. • Typical stimulation occurring during induction of anesthesia includes laryngoscopy and intubation, which constitute profoundly noxious stimuli. • Frequently, response to these two procedures cannot be eliminated completely with just the intravenously administered hypnotic.
Thus, assessment of the depth of anesthesia with the use of clinically relevant noxious stimuli such as laryngoscopy and intubation requires the concurrent administration of other analgesic drugs (opioids or nitrous oxide) to provide reasonable and clinically acceptable hemodynamic control.