Download
1 / 23
230 likes | 328 Views
Contributions to TSC1 & 2 Gene Variation Databases. 0.5%. [Single Queries]. 3%. 3%. 6%. 4%. 0.05%. [Parents]. 17%. 18%. Unpublished data Total = ~25%. Unpublished data Total = 27%. Published data 73%. Published data 75%. TSC1 N=820 entries. TSC2 N*=2064 entries.

E N D
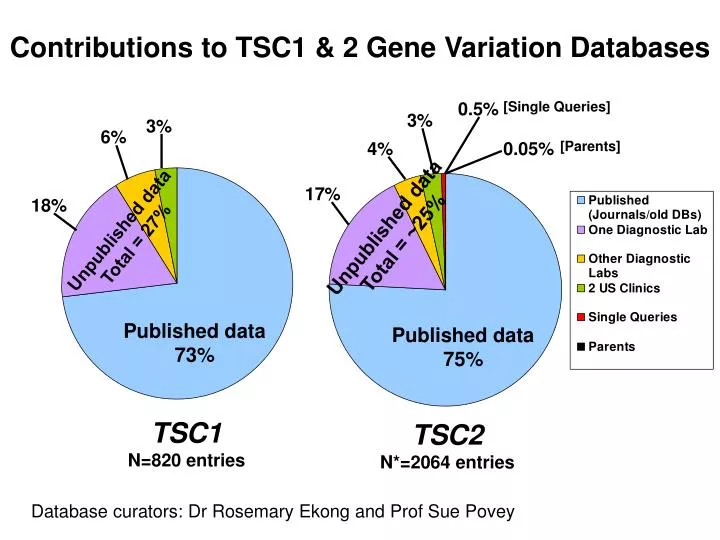
Contributions to TSC1 & 2 Gene Variation Databases 0.5% [Single Queries] 3% 3% 6% 4% 0.05% [Parents] 17% 18% Unpublished data Total = ~25% Unpublished data Total = 27% Published data 73% Published data 75% TSC1 N=820 entries TSC2 N*=2064 entries Database curators: Dr Rosemary Ekong and Prof Sue Povey
A phase II trial of the mTOR inhibitor sirolimus in patients with TSC or sporadic LAM (TESSTAL trial) Julian Sampson, Institute of Medical Genetics, Cardiff, UK See Davies DM et al. Clin Cancer Res 2011; 17:4071-4081
Current and Completed Clinical Trials of mTOR inhibition in TSC 8 Barcelona 18 AML sirolimus II 9 Cincinnati/Houston 20 Seizures everolimus II 10 Boston/Cincinnati 20 Neurocognition everolimus II 11 Cincinnati 99* LAM everolimus II
TESSTAL: Design • Non-randomised, Open label • Multicentre (Brighton, Cardiff, Nottingham, Zurich) • Primary outcome = angiomyolipoma size • Oct 2005 – Sept 2009 • Fleming’s single stage design • P1 0.1, P2 0.4, α 0.05, β 0.1 (N ≥ 15) • Sample size: 16 recruited • Intention to treat
Treatment • Oral sirolimus as liquid, once daily for 2 years • Dose adjusted to obtain: - Starting drug level 3-6 ng/ml - Escalation to 6-10 ng/ml at 2 months (first MRI on treatment) unless all target AML reduced by ≥ 10% (4 of 16 patients) • Sirolimus levels lower than in previous trial (Bissler et al.)
Major Inclusion Criteria TSC (Roach criteria, 1998) or LAM (CT/Bx) 1 or more AML of ≥ 2cm 18 – 65 yrs of age GFR ≥ 40 mL/min Major Exclusion Criteria IQ < 70 AML bleed last 12 months AML embolization last 6 months Continuous O2 requirement Proteinuria >1g/day Pregnancy/intention Breast-feeding Change in AED in last 3 months
Assessments: Primary Outcome • AML size by serial MRI scan • Un-enhanced transaxial scans, 1.5 Tesla systems • Scans at baseline, 2, 6,12, 24 months • Up to 5 target AMLs per kidney • Sum Longest Diameters (SLD) • RECIST criteria i.e. response is ≥ 30% reduction in SLD and no new lesions
Assessments: Secondary Outcomes • Pulmonary Function • FEV1, FVC, DLCO at baseline,4, 6, 12, 24 months • Expressed as % predicted values • Neurocognition • IQ for inclusion by NART • Immediate recall memory - AIMBP • Immediate recognition memory - CANTAB • Executive function - CANTAB
19 patients with tuberous sclerosis or lymphangiomeiomatosis (LAM) screened 3 were not enrolled 2 were ineligible 1 declined to participate 16 patients enrolled 6 had LAM only 3 had tuberous sclerosis and LAM 7 had tuberous sclerosis only 9 with LAM had pulmonary function assessed at baseline 14 had neurocognitive assessment at baseline 16 had angiomyolipomas measured at baseline SIROLIMUS THERAPY, 16 started 15 had angiomyolipomas measured at 2 months 1 withdrew 8 had pulmonary function assessed at 4 months 13 had neurocognitive assessment at 4 months 1 withdrew 6 had pulmonary function assessed at 6 months# 13 had angiomyolipomas measured at 6 months* 1 withdrew 11 had neurocognitive assessment at 12 months 6 had pulmonary function assessed at 12 months# 12 had angipomyolipomas measured at 12 months 1 withdrew 1 withdrew 1 died 5 had pulmonary function assessed at 24 months 10 had angiomyolipomas measured at 24 months
19 patients with tuberous sclerosis or lymphangiomeiomatosis (LAM) screened 3 were not enrolled 2 were ineligible 1 declined to participate 16 patients enrolled 6 had LAM only 3 had tuberous sclerosis and LAM 7 had tuberous sclerosis only 9 with LAM had pulmonary function assessed at baseline 14 had neurocognitive assessment at baseline 16 had angiomyolipomas measured at baseline SIROLIMUS THERAPY, 16 started 15 had angiomyolipomas measured at 2 months 1 withdrew 8 had pulmonary function assessed at 4 months 13 had neurocognitive assessment at 4 months 1 withdrew 6 had pulmonary function assessed at 6 months# 13 had angiomyolipomas measured at 6 months* 1 withdrew 11 had neurocognitive assessment at 12 months 6 had pulmonary function assessed at 12 months# 12 had angipomyolipomas measured at 12 months 1 withdrew 1 withdrew 1 died 5 had pulmonary function assessed at 24 months 10 had angiomyolipomas measured at 24 months
19 patients with tuberous sclerosis or lymphangiomeiomatosis (LAM) screened 3 were not enrolled 2 were ineligible 1 declined to participate 16 patients enrolled 6 had LAM only 3 had tuberous sclerosis and LAM 7 had tuberous sclerosis only 9 with LAM had pulmonary function assessed at baseline 14 had neurocognitive assessment at baseline 16 had angiomyolipomas measured at baseline SIROLIMUS THERAPY, 16 started 15 had angiomyolipomas measured at 2 months 1 withdrew 8 had pulmonary function assessed at 4 months 13 had neurocognitive assessment at 4 months 1 withdrew 6 had pulmonary function assessed at 6 months# 13 had angiomyolipomas measured at 6 months* 1 withdrew 11 had neurocognitive assessment at 12 months 6 had pulmonary function assessed at 12 months# 12 had angipomyolipomas measured at 12 months 1 withdrew 1 withdrew 1 died 5 had pulmonary function assessed at 24 months 10 had angiomyolipomas measured at 24 months
19 patients with tuberous sclerosis or lymphangiomeiomatosis (LAM) screened 3 were not enrolled 2 were ineligible 1 declined to participate 16 patients enrolled 6 had LAM only 3 had tuberous sclerosis and LAM 7 had tuberous sclerosis only 9 with LAM had pulmonary function assessed at baseline 14 had neurocognitive assessment at baseline 16 had angiomyolipomas measured at baseline SIROLIMUS THERAPY, 16 started 15 had angiomyolipomas measured at 2 months 1 withdrew 8 had pulmonary function assessed at 4 months 13 had neurocognitive assessment at 4 months 1 withdrew 6 had pulmonary function assessed at 6 months# 13 had angiomyolipomas measured at 6 months* 1 withdrew 11 had neurocognitive assessment at 12 months 6 had pulmonary function assessed at 12 months# 12 had angipomyolipomas measured at 12 months 1 withdrew 1 withdrew 1 died 5 had pulmonary function assessed at 24 months 10 had angiomyolipomas measured at 24 months
Angiomyolipoma Response sum of longest diameters • Reduction AML burden in all patients • 8/16 patients respond by RECIST criteria • 8/10 in per-protocol group • 25% diameter reduction ≡ 60% in volume (for spherical lesions)
AML Response • 41 / 48 AMLs smaller at last measurement than baseline • 2 unchanged • 5 larger: TSC3 - 1 of 5 AMLs increased by 1mm. Others shrank by 20-30% TSC4 - 4 of 9 AMLs grew (by up to 30%) while 5 shrank (by up to 25%) • Most shrinkage in first year – mean LD of AMLs measured at 0,12 and 24 months were 2.92, 2.19 and 2.11cm respectively
Lung Function in Patients with LAM Mean rate of decline in FEV1 = 49 ml/yr over 12/12 (N=7) = 76 ml/yr over 24/12 (N = 5)
IQ and Neurocognitive Deficits TSC* N S-LAM N IQ (SD) 105 (+/-15)8107 (+/-12)6 Deficits on Tests (< 5th Percentile) At Baseline 9/88 (10.2%) 82/63 (3.2%) 6 At 4 months 6/88 (6.8%)81/45 (2.2%) 5 At 12 months 7/77 (9.1%)70/44 (0%) 5 * No patient with TSC had seizures in the year prior to or during the study
Neurocognitive Tests: Summary Scores by Domain Immediate Recall Memory TSC mean change + 2 S-LAM +1.6 Immediate Recognition Memory TSC mean change -1.625 S-LAM - 0.6 Executive Function TSC mean change + 1.5 S-LAM + 3.0
Adverse Events • Reported in all patients. Majority CTCAE grade 1 or 2 • All patients had some time off therapy (days to months) • Drug discontinued in 2 patients because of toxicity (peripheral oedema, proteinuria) • One death (deemed unrelated to treatment) • Frequent AEs: Respiratory infections, 5/16 – all LAM 3 serious and possibly sirolimus-related Mouth ulcers, 6/16 Proteinuria, 5/16
Summary • Sirolimus therapy (3-10ng/ml) reduced size of most AMLs in patients with TSC or S-LAM • AML burden reduced in all patients • Most shrinkage in first year of therapy • Response sustained at 2 years • Side effects acceptable to most patients – but care in LAM • Neurocognitive function – similar changes in TSC and S-LAM patients • Lung function in LAM – little change, decline slowed ?
Acknowledgements TESSTAL team: D Mark Davies, Petrus de Vries, Simon Johnson, Deborah McCartney, Jane Cox, Andreas Serra, Peter Watson, Christopher Howe, Tim Doyle, Kate Pointon, Justin cross, Anne Tattersfield, Chris Kingswood. J Bissler, D Franz, D Kruger, F McCormack (Cincinnati) A Hunt TSA, James Tudor Trust, Wyeth (Pfizer)
TRON: UK Trial of Everolimus for neurocognitive problems in TSC
TRON • Randomized control (2:1) trial, single UK centre • Recruitment target 48 • Age 16 - 60 yrs • IQ ≥ 60 and deficit (-2 SD or more) in a 1º outcome measure • 6 months treatment, blood levels 3-10ng/ml • Determine effect sizes on recall memory and executive function in TSC • Secondary outcomes: seizures, QOL, wider aspects of neurocognition, safety • Protocol developed with Novartis and TSA (GB) • Recruitment planned to open end 2011