Download
1 / 34
370 likes | 705 Views
Tumors of Nose and PNS. Dr Deekshith RM Senior resident YMC 17/01/2019. Headache. Facial Pain. Trigeminal Neuralgia: a sudden, usually unilateral, severe, brief, stabbing, recurrent pain in the distribution of one or more branches of the fifth cranial nerve Temporomandibular disorder

E N D
Tumors of Nose and PNS Dr Deekshith RM Senior resident YMC 17/01/2019
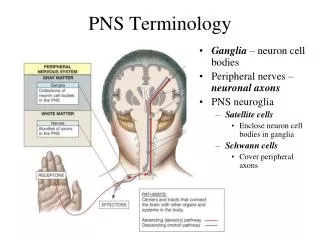
Facial Pain • Trigeminal Neuralgia: a sudden, usually unilateral, severe, brief, stabbing, recurrent pain in the distribution of one or more branches of the fifth cranial nerve • Temporomandibular disorder • Acute rhinosinusitis
Squamouspapilloma • C/F • Papilloma • Bleeding • Mass • Biopsy • Treatment: excision with cautery
Inverted papilloma (Transitional cell papilloma or Ringertztumour or Schneiderianpapilloma). • Non olfactory mucosa of nose (Schneiderian membrane) and paranasal sinuses. • Most common site of origin is lateral wall of nose in the middle meatus; less commonly it arises from the maxillary, frontal or sphenoid sinus • HPV association • C/F proptosis, nasal mass,epistaxis, nasal obstruction • CT/MRI: • Rx: Medial Maxillectomy
Sinonasal Malignancy • Sinonasal malignancies have an incidence of 05-1 per 100,000 per year. • They account for 0.2-0.8 %of all malignancies and 3 %of upper aerodigestive tract neoplasms. • Most develop in the fifth and sixth decades of life. • The incidence in men is twice that of women
Workers exposed to Hard wood have a 70 times increased incidence of sino nasal Adenocarcinoma, particularly in the Ethmoid sinuses. • Soft wood exposure increases the risk of developing Squamous cell carcinoma. • exposure to nickel- sino nasal squamous cell carcinoma 250 times. • chromium, polycyclic hydrocarbons, aflatoxin (found in certain foods and dust), mustard gas and thorotrast (thorium dioxide used in paints for watch dials). • Radiation, viral and genetic causes
maxillary sinus tumours (55 percent) • Nasal cavity (35 percent), • ethmoid sinuses (9 percent) and • rarely • frontal and sphenoid sinuses (1 percent).
Clinical features antral ethmoid • Nasal obstruction • Epistaxis • Infraorbital anesthesia • Toothache • Facial pain • trismus • Nasl obstruction • Epistaxis • Proptosis/diplopia
Computed Tomography: • Magnetic Resonance Imaging • Angiography • Positron Emission Tomography • Biopsy
Maxillary Sinus Tumors • Early (T1 and T2) lesions may be treated by surgical resection (maxillectomy) or irradiation • irradiation alone (5500 rad) • As stated previously, most investigators agree that T3 and T4 lesions require combined therapy.
Combined Irradiation and Surgery • With T3 tumors, there is little survival difference between preoperative irradiation and postoperative irradiation • Postoperative irradiation often controls microscopically positive resection margins. • With the more advanced lesions, especially those for which resectability is questionable, preoperative irradiation appears to be the procedure of choice
Radiotherapy • Chemotherapy: topical 5-flurouracil for SCC & AdenoCA • Endoscopic resection is palliative
Squamous cell carcinoma • Squamous cell carcinoma (SCC) is the most common • The highest incidence is in the seventh decade of life and there is a male preproderence • Arise from lateral wall with 50%on the turbinates. Two-thirds of septal SCC are found anteriorly in the region of the mucocutaneous junction. Ca of columella is most aggressive form. • Transformation of Schneiderianpapillomas into SCC is a recognized risk 14.6 percent incidence. • Papillary and exophytic histological patterns
Macroscopically: • some sino nasal squamous cell carcinomas have a polypoid appearance, while others are more obviously fungating, friable and keratinizing. • Approximately 85 percent of SCC are well differentiated and keratinizing tumours.
Management • SCC: For the treatment of early lesions, surgery, if the tumor is excised en bloc with good margins, and, if there is no evidence of perineural spread, then surgery is usually sufficient. If there are any questions about the margins or perineural invasion, the addition of radiation is indicated External Inferior medial Medial Radical
Management • There has been some literature reporting the use of radiation therapy alone for early disease, but this is not necessarily recommended since radiation of this side of the body has significant morbidity, with possible osteoradionecrosis and vision loss as well as damage to the spinal cord. • Combined modality generally tends to be the gold standard: surgery with postoperative radiation therapy.
Adenoid cystic carcinoma • A little less than 5 percent of sino nasal malignancies are adenoid cystic carcinomas (ACC). • As elsewhere, ACC tend to grow slowly but inexorably with early perineural and vascular spread. All variants of the tumour are seen. • nerves involved are: infraorbital,maxillary, greater palatine and sphenopalatine. • The maxillary sinus is the most commonly affected site and patients usually present with a long history of facial pain that has defied diagnosis for many months if not years
Several histological subtypes of sino nasal adenocarcinoma • namely papillary, sessile, mucoid, neuroendocrine, intestinal and undifferentiated. • Papillary adenocarcinomastend to be locally malignant only and are the least aggressive form. • The intestinal variety is most often associated with woodwork-induced tumours. • Sessile and mucoidadenocarcinomas have the worst prognosis
Management • Adenocarcinoma: Treatment is controversial, but the literature indicates that craniofacial resection is the key.
Esthesioneuroblastoma • Also called olfactory placodetumour as it arises from the • olfactory epithelium in the upper third of nose. • Bimodal peaks of incidence at 10–20 and 50–60 years are seen. • Most common symptoms are unilateral nasal obstruction and epistaxis. • When tumour invades orbit and the surrounding structures, other symptoms like proptosis, headache, epiphora, diplopia and blurred vision can also arise. • Lymph node metastases in the neck can occur in 10–15%. • Intranasal or endoscopic examination of nose reveals a friable cherry-red, polypoidal mass in the upper third of nasal cavity. • It is a vascular tumour and biopsy should not be immediately attempted unless imaging studies have been done.
Patients with OAN causing Cushing's syndrome, inappropriate antidiuretic hormone secretion or hypertension produced by vasoactive peptide. • four-point histological grading system for OAN based on such features as the • degree of differentiation, the tumour architecture, mitotic index, nuclear polymorphism, fibrillary nature of the matrix and tumour necrosis.
(a) Craniofacial resection with adjuvant radiation. • (b) Preoperative radiation followed by craniofacial resection. • (c) Preoperative chemotherapy and radiation followed by craniofacial resection for advanced lesions extending to orbit, cribriform plate and intracranially. • Neck nodes if present are also radiated.
Hemangiopericytoma • Arises from Pericytes ( Zimmerman) of outer capillary wall • They account for less than 5 percent of all sarcomas. Within the head and neck, • Present as rubbery, pale/gray, well circumscribed lesions resembling nasal polyps
HISTOPATHOLOGY: • Proliferation of capillaries surrounded by connective tissue sheath • Silver stain blackens the sheath of capillaries allowing accurate demonstration of malignant cells at periphery • Treatment is surgical resection with postoperative XRT for positive margins but radio resistant (recurrence 10-60%)
Lymphoma. • Plasmacytoma. • Sarcomas.
SUMMARY • Headache and Facial Pain • Tumors of Nose and PNS
References • Scott Brown • DINGRA • Internet