Download
1 / 15
170 likes | 346 Views
Pooled analysis of clinical outcomes in studies of patients with EGFR mutations treated with either an EGFR TKI or chemotherapy. Luis Paz-Ares 1 , Denis Soulières 2 , Barbara Klughammer 3 , Ivan Melezínek 4 , Joachim Moecks 5 , Tony Mok 6

E N D
Pooled analysis of clinical outcomes in studies of patients with EGFR mutations treated with either an EGFR TKI or chemotherapy Luis Paz-Ares1, Denis Soulières2, Barbara Klughammer3, Ivan Melezínek4, Joachim Moecks5, Tony Mok6 1Hospital Universitario Virgen del Rocío, Seville, Spain; 2Centre Hospitalier de l’Université de Montréal, Montréal, Canada; 3F. Hoffmann-La Roche Ltd, Basel, Switzerland; 4Roche Products Ltd, Welwyn Garden City, UK; 5BIOMCON GmbH, Mannheim, Germany; 6The Chinese University of Hong Kong, Prince of Wales Hospital, Hong Kong, China
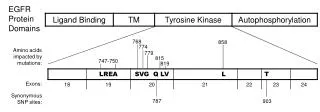
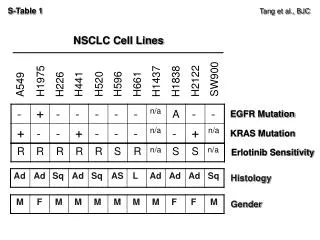
EGFR mutations Exons EGFR • Activating mutations • exon 19 deletion • L858R • Overall incidence in population • ~10% in Western countries • ~30% in Asian countries 18 G719X 3.2% P-loop 19 Deletion 48.2% C helix 20 Insertion Kinase domain K 3.7% 21 L858R A-loop 42.7% Mitsudomi T, et al. Int J Clin Oncol 2006
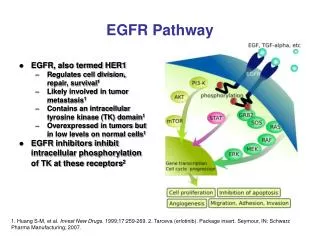
Biological significance of EGFRmutation-positive NSCLC • EGFR TK mutations have significant biological consequences • constitutive activation of receptor • preferential dimerisation with HER3, leading to strong AKT / STAT survival pathway signalling • tumours may be ‘addicted’ to this signalling • EGFR inhibition may be essential to restore apoptosis • Opportunity for personalised treatment of NSCLC Sordella R, et al. Science 2004
Clinical characteristics of EGFR mutation-positive NSCLC – SLCG Data
Optimal treatment outcomes: EGFR TKI or chemotherapy? • Limited prospective data in EGFR mutation+ NSCLC • most existing data from small, retrospective studies, often limited to single ethnic groups • Challenges for prospective studies • relatively low rate of mutations • limited availability of tumour samples • Pooled analysis performed to consolidate available data • provide broad overview of data across different clinical settings and ethnicities
Methodology • Searches performed using major databases(to 11 June 2009) • PubMed, Embase, Biosis Previews • excluded reviews and non-English language • included data from ASCO 2008 and 2009 • Inclusion criteria • median PFS/TTP reported for patients with EGFR mutations who received chemotherapy or EGFR TKI monotherapy (any line of treatment), with associated sample size • Exclusion criteria • two EGFR TKIs studied in sequence • EGFR TKI given as maintenance or adjuvant therapy • data reported in another publication (latest update was included)
Statistical approach Methods • Weighted estimate of pooled median PFS • Accuracy interval based on exponential distribution • Bootstrap re-sampling to check accuracy interval • Permutation testing to compare median PFS estimates between treatments • Potential publication bias addressed Limitations of this analysis • No individual patient data • only high level information, no account for censored observation • Considers only PFS • non-standardised PD assessment across studies • Due to reporting differences, individual mutations not considered separately • No restriction on study designs or study quality
Reports identified from broad literature search (n=564) Studies identified from ASCO 2008–9 search (n=42) Excluded based on abstract or title: no clinical data related to question (n=431) Studies retained for full paper review (n=175) • Excluded (n=121) • PFS/TTP/n not reported for pts with mutations (n=96) • EGFR TKIs given sequentially or as maintenance or adjuvant therapy (n=10) • Data duplicated in another publication (n=15) Studies included (n=54) Summary of search strategy
Total number of patients = 1,809 (65% treated in first-line setting) Summary of data included
Median PFS from individual studies90% accuracy intervals(any line of therapy) Erlotinib Gefitinib Chemotherapy
Pooled analysis(any line of therapy) Pooled median PFS(95% accuracy interval) 13.2 (12.0–14.7) 9.8 (9.2–10.4) 5.9 (5.3–6.5) Permutation test for estimated pooled median PFS (1,000 iterations) EGFR TKI vs chemotherapy p=0.000 (two-sided)
Analysis to assess publication bias • Spread of data suggests no publication bias Chemotherapy Gefitinib Erlotinib
Conclusions • This analysis suggests longer PFS with erlotinib (13.2 months) and gefitinib (9.8 months) than chemotherapy (5.9 months) in EGFR mutation+ NSCLC • Magnitude of benefit adds to evidence that EGFR TKIs should be the preferred first-line option in EGFR mutation+ disease • avoids toxicity of chemotherapy • many patients do not receive second-line therapy due to worsening condition • Prospective studies are essential to confirm these findings
Ongoing prospective first-line studies in patients with EGFR mutation+ NSCLC • EURTAC (Europe) • phase III, randomised (n=173) • erlotinib 150mg/day vs platinum doublet • OPTIMAL, ML20981 (China) • phase II, randomised (n=150) • erlotinib 150mg/day vs platinum doublet • WJTOG 3405 (Japan) • phase III, randomised • gefitinib 250mg/day vs cisplatin/docetaxel Primary endpoint in all trials: PFS