Download
1 / 51
540 likes | 986 Views
Role of MRI in Assessment and Diagnosis of Axial Spondyloarthritis Lebanese Society of Rheumatology 2009 Nov 07 Ulrich Weber MD, Rheumatology Balgrist University Hospital, Zurich, Switzerland. Disclosure. Nothing to disclose No advisory board memberships

E N D
Role of MRI in Assessment and Diagnosis of Axial Spondyloarthritis • Lebanese Society of Rheumatology 2009 Nov 07 • Ulrich Weber MD, Rheumatology • Balgrist University Hospital, Zurich, Switzerland
Disclosure • Nothing to disclose • No advisory board memberships • Funding of the project Whole Body MRI in SpA • Walter L. and Johanna Wolf Foundation, Zurich, Switzerland • Foundation for Scientific Research at the University of Zurich, Switzerland
Ankylosing SpondylitisNonaxial Disease Dactylitis Uveitis Coxitis Anterior chest wall inflammation
Objectives • Role of MRI in early diagnosis of axial SpA • Whole body MRI – a promising MRI variant • Emerging roles of MRI in axial SpA
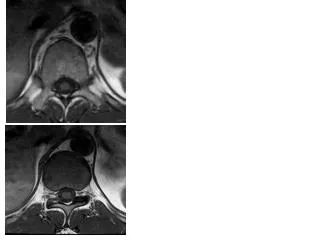
Early diagnosis28y f, fall from horse 15 mo ago, persist. LBP
Early diagnosis28y f, fall from horse 15 mo ago, persist. LBP
Ankylosing SpondylitisDelayed diagnosis • Germany 1999 8.8 years • Switzerland 2005-2008 5.7 years Feldtkeller E et al. Rheumatol Int 2003;23:61 SCQM AS; Zollikofer A. Medical thesis (unpublished data)
SpA - The challenge of early diagnosis • Early SpA • No validated diagnostic criteria • Plain radiography • Equivocal findings in early SpA • Definite lesions are seen after ~10 years Rudwaleit M et al. Arthritis Rheum 2005;52:1000 Mau W et al. J Rheumatol 1988;15:1109
Radiographic SIJ classification grade 1/2 grade 2 grade 3 grade 4 Van der Linden S et al. Arthritis Rheum 1984;27:361
Radiographic SIJ classification Moderate sensitivity and specificity • Scoring of SIJ by23 radiologists and 100 rheumatologists • Sensitivity 84 % / 80 % Specificity 71 % / 75 % • After training unchanged • Sensitivity 83 % / 79 % Specificity 80 % / 76 % Van Tubergen A et al. Ann Rheum Dis 2003;62:519
Modified New Yorkclassification criteria • low back pain >3 months‘ duration improved by exercise and not relieved by rest • limited lumbar spinal motion in both the sagittal and frontal planes • decreased chest expansion (rel. to normal values for sex and age) • bilateral radiographic sacroiliitis grade 2–4 • unilateral radiographic sacroiliitis grade 3–4 • Positive: 1 of 2 radiographic AND ≥1 of 3 clinical criteria Van der Linden S et al. Arthritis Rheum 1984;27:361
ASAS classification criteria for axial SpA Sacroiliitis on imagingX-ray or MRI plus ≥1/11 clinical features IBP; Arthritis; Enthesitis (heel); Uveitis; Dactylitis; Ps/CD/UC; HLAB27; Response to NSAIDs; FH SpA; CRP Sensitivity 66% Specificity 97% „Imaging arm“ HLA B27 plus ≥2/10 clinical features IBP; Arthritis; Enthesitis (heel); Uveitis; Dactylitis; Ps/CD/UC; Response to NSAIDs; FH SpA; CRP Sensitivity 83% Specificity 84% „Clinical arm“ Rudwaleit M et al. Ann Rheum Dis 2009;68:777 n = 649 pat; LBP >3 mon; symptom onset <45 J; rheumatology practices
ASAS classification criteria for axial SpA • MRI equivalent to plain X-ray • however: • What is a positive MRI? • in the spine? • in the SIJ?
Diagnostic utility of spinal MRI lesions • Romanus Lesion (RL)= Spondylitis angularis • ≥3 RL: positive LR 12 1 • ≥2 RL: positive LR 12 2 Clinical relevance LR+: 3 5-10 moderate >10 high 1Bennett AN et al. Arthritis Rheum 2009;60:1331 2Weber U et al. Arthritis Rheum 2009;61:900 3Jaeschke R et al. JAMA 1994;271:703
SpA ? • „Romanus-Lesion“ in 26% of healthy volunteers Weber U et al. Arthritis Rheum 2009;61:900
Diagnostic utility of chronicspinal MRI lesions STIR T1 • Fatty Romanus Lesion • >0 FRL: positive LR 5 • >5 FRL: positive LR 13 Bennett AN et al. Ann Rheum Dis 2009;published online 9 Aug
Diagnostic utility of SIJ MRI lesionsASAS/OMERACT consensual approach • Active inflammatory SIJ lesions required • Subchondral or periarticular bone marrow edema (BME) highly suggestive of sacroiliitis • BME score ≥2 on a single SIJ slice and/or ≥1 lesion on 2 consecutive slices 1 slice sufficient require 2 slices Rudwaleit M et al. Ann Rheum Dis 2009;68:1520
What about structural lesions? T1 Erosions STIR Symptom duration 24 months; normal pelvic X-ray
Diagnostic utility of SIJ MRI lesions MORPHO Study 4 abstracts EULAR 2009 Copenhagen 5 abstracts ACR 2009 Philadelphia
Objectives of MORPHO program • To assess the diagnostic utility of SIJ MRI by - MRI sequences used in routine practice - comparison with appropriate controls • To assess the relative contribution of T1 (structural lesions) versus STIR (acute lesions) to assess diagnostic utility • To define a „positive“ MRI for SpA using a data driven approach
MORPHO Methodology 187 subjects / patients All ≤45 years old All patients with inflammatory back pain≤10 years duration Subjects 59 asymptomatic healthy volunteers (HV) 26 patients with non-specific back pain (NSBP) 77 patients with SpA (met modified NY criteria) 25 patients with inflammatory back pain (did not meet modified NY criteria)
MORPHO Methodology Erosion Bone Marrow Oedema T1 STIR Ankylosis Fatty Infiltration T1 T1
MORPHO resultsMean Sens, Spec and LR+/- for 5 readers AS: Ankylosing spondylitis IBP: Inflammatory back pain = Preradiographic SpA NSPB: Non-specific back pain HC: Healthy controls
Diagnostic utility of SIJ MRI lesionsMORPHO proposal • BME score ≥2 on a single SIJ slice and/or≥1 on 2 consecutive slices (ASAS proposal) • OR • Erosion score ≥2 on a single SIJ slice or ≥2 on 2 consecutive slices • OR • BME score ≥1 ANDErosion score ≥1 on any slice
IBP patients: Comparison of diagnostic utilityASAS versus MORPHO proposal ASAS proposal MORPHO proposal NB: 13/25 (52%) IBP patients diagnosed as SpA by ≥2 readers according to overall assessment of MRI
SpA ?Bone marrow edema-like lesion STIR T1 35y old healthy volunteer
SpA ?Fat deposition STIR T1 Healthy volunteer
SpA ?Erosion- and BME-like lesion STIR T1 Healthy volunteer
Inflammatory back pain and SpAMRI – the key for early diagnosis • Suspicion based on clinical grounds(IBP / additional clinical SpA features) • Plain X-ray of the pelvis • Radiographic („late stage“) SpA • MRI (conventional or whole body) • Preradiographic („early“) SpA Heuft-Dorenbosch L et al. Ann Rheum Dis 2006;65:804
Objectives • Role of MRI in early diagnosis of axial SpA • Whole body MRI – a promising MRI variant • Emerging roles of MRI in axial SpA
WB MRI – a recently introduced imaging modality Multichannel technology Parallel imaging Whole body multicoil systemSpatial resolution WB = CON MRI Fusion of the imagesby a dedicated software Moving table platformNo patient or coil repositioning
WB MRI in ASPractical issues • Examination time30 minutes including patient positioning • Reporting time15 minutes for a trained reader • Costsabout 1.5 times the expense for CON MRI(in billing systems based on the amount of time needed for a particular exam) • Additional imaging of lower extremitiespotential objective measure for enthesitisadditional examination time of 20 minutes
WB MRI – introduced for systemic screening in oncology and angiology Oncological screening and staging Systemic arterial occlusive disease Nael K et al. AJR 2007;188:529-39 Schaefer JF et al. Eur Radiol 2006;16:2000-15
Validation Whole body MRI versus Conventional MRI in SpA: SIJ and spine Weber U et al. Ann Rheum Dis 2009;published online 7 MayWeber U et al. Arthritis Rheum 2009;61:893
MRI lesions in early SpA21y m, HLA B27+, IBP 14 months, ESR 55
Early diagnosis in monozygotic twin23y m, dactylitis, right buttock pain for 4 mo September 2008 August 2007 Diagnosis 4 months after symptom onset Weber U et al. J Rheumatol 2008;35:1464
WB MRI in clinical practiceCoxitis 30 yrs old male, disease duration 7 yrs; no hip pain
WB MRI in clinical practice Inflammatory versus mechanical back pain Pseudarthrosis T10/11 after transspinal fracture • 57 yrs old male, HLA B27+, disease duration 32 yrs, fusion th/l spine • Increasing th/l back pain for 3 yrs, intense night pain • no response to conventional and alternative therapy Weber U, Maksymowych WP. Skelet Radiol 2008;37:487-90
Objectives • Role of MRI in early diagnosis of axial SpA • Whole body MRI – a promising MRI variant • Emerging roles of MRI in axial SpA
Inflammatory MRI spinal lesions Predictive for new syndesmophytes • Prospective observational cohort, follow-up after 24 months by plain X-ray and MRI • New syndesmophytes developed significantly more frequently in vertebral corners with inflammation (14.3%) than in those without inflammation (2.9%) seen on baseline MRI (p<0.003) Maksymowych WP et al. Arthritis Rheum 2009;60:93 Baraliakos X et al. Arthritis Res Ther 2008;10:R104
Guiding TNFa-inhibitor treatment in early SpA (symptom duration 3mo-3y) • Percentage of ASAS partial remission • Early SpA (MRI) 55.6% 1 • Established SpA (Xray) 22.4% 2 1Barkham N et al. Arthritis Rheum 2009;60:946 2Van der Heijde D et al. Arthritis Rheum 2005;52:582
Monitoring response to TNFa-inhibitors 2006 2009
Disease activityMRI versus clinical/laboratory parameters • No correlation of MRI activity parameters with clinical and laboratory activity in various study designs (cross-sectional, cohort and interventional studies) • MRI may reflect other aspects of disease activity than the ones expressed by clinical and laboratory parameters Puhakka KB et al. Rheumatology 2004;43:234Maksymowych WP et al. Arthritis Rheum 2007;57:501Lambert RG et al. Arthritis Rheum 2007;56:4005Weber U et al. Arthritis Rheum 2009;61:893
Roles of MRI in axial SpASummary • Confirmation of SpA diagnosis suspected on clinical grounds (preradiographic stage) • Diagnostic MRI thresholds both for SIJ and spine needed • Emerging role for guiding treatment andpredicting disease course
Acknowledgement Radiology Balgrist Juerg Hodler Marco Zanetti Christian Pfirrmann Rheumatology Balgrist Rudolf Kissling Walter Maksymowych, Edmonton Robert Lambert, Edmonton Anne Grethe Jurik, Aarhus Anna Zejden, Aarhus Mikkel Ostergaard, Copenhagen Susanne Pedersen, Copenhagen Asim Khan, Cleveland Kaspar Rufibach, Zurich Rahel Kubik, Baden Stefan Duewell, Frauenfeld
Discussion White-browed Robin (pair)