Download
1 / 15
150 likes | 272 Views
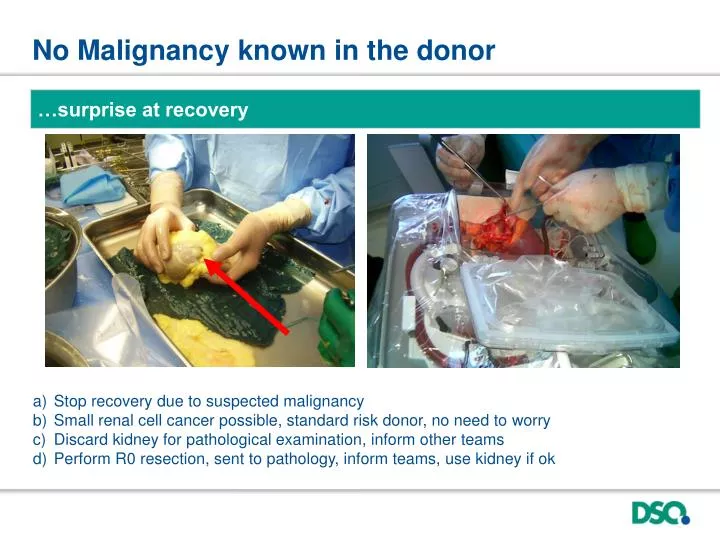
No Malignancy known in the donor. …surprise at recovery. Stop recovery due to suspected malignancy Small renal cell cancer possible, standard risk donor, no need to worry Discard kidney for pathological examination, inform other teams

E N D
No Malignancy known in the donor …surprise at recovery • Stop recovery due to suspected malignancy • Small renal cell cancer possible, standard risk donor, no need to worry • Discard kidney for pathological examination, inform other teams • Perform R0 resection, sent to pathology, inform teams, use kidney if ok
No Malignancy known in the donor …surprise at recovery In any suspect lesion malignancy must be ruled out (histology), inform every team ! R0 resection of renal mass < 1.0 cm (kidney may be used if no renal cell cancer is confirmed ) ! Remove always fat tissue around kidney without capsule lesion and damage to no touch area ! -> infarct, not older than 24 hours. Kidney was transplanted & all other organs too.
24 yr., female, brain death after cardiac arrest head ache, psychosis since 2 weeks after oral drug abuse (recreational drugs), trip to India 3 months ago, treated for psychosis….brain death (cardiac resuscitation, severe brain edema, EF 20%) • Cardiac reason for brain death -> all other organs may be used • Recreational drug abuse caused complication -> organs may be used • Unclear situation, stop recovery
24 yr., female, brain death after cardiac arrest head ache, psychosis since 2 weeks after oral drug abuse (recreational drugs), trip to India 3 months ago, treated for psychosis….brain death (cardiac resuscitation, severe brain edema, EF 20%) • ECD, coordinator insisted on autopsy • ~ 4 weeks: brain-stem encephalitis possible, no myocarditis • ~ 6 weeks: neurological alteration in two recipients • ~ 2nd look donor brain -> -> RT-PCR: Rabies • third source information: “a dog scratched her…” • Try to obtain information as much as possibel !!! donor brain IF-Antibody recipient brain IF-Antibody Remember: any uncertain encephalitis is a contraindication until you know the pathogen !
8 months, boy, head injury, brain death • Donor: • head trauma, neurosurgery, 10 transfusions (72-48 hrs. ago), brain death, consent…Leucos., CRP, platelets • Mother: • pregnancy in Africa • Father: • suspected drug abuse, Africa Questions • Sepsis -> stop • Riskofuntreatabletropicalinfections -> stop • Problems shouldbefurtherinvestigated • Standard riskdonor, noproblem
8 months, boy, head injury, brain death • Donor: • head trauma, neurosurgery, 10 transfusions (72-48 hrs. ago), brain death, consent…Leucos., CRP, platelets • Mother: • pregnancy in Africa • Father: • suspected drug abuse, Africa Solution Mother: 1st-7th mo. of pregnancy in South Africa anti-HIV neg, anti-HCV neg, HBsAg neg, anti-HBc neg sanitary living conditions, no animal contacts Father: alcohol problem, therefore divorced
8 months, boy, head injury, brain death • Donor: • head trauma, neurosurgery, 10 transfusions (72-48 hrs. ago), brain death, consent…Leucos., CRP, platelets • Mother: • pregnancy in South Africa (1st-7th month), Virology o.k. • Father: • Alc., South-Africa (well urbanized) Which organs (80cm, 11kg) ? • Heart, liver, kidney • Heart, lung, liver, kidney • Heart, lung, liver, intestine, kidney • Heart, lung, liver, intestine, pancreas, kidney
8 months, boy, head injury, brain death • Donor: • head trauma, neurosurgery, 10 transfusions (72-48 hrs. ago), brain death, consent…Leucos., CRP, platelets • Mother: • pregnancy in South Africa (1st-7th month), Virology o.k. • Father: • Alc., South-Africa (well urbanized) Which organs (80cm, 11kg)? • Heart, liver, kidney, smallbowel+colontransplanted • Lung, pancreas: nocentreaccepted • Considermultivisceral-packageforsmallchilds
67 yr., 4 days ago cardiac resuscitation (45 min) • absolute Arrhythmia, norepinehrine, anuria, haemoflitration (4 days) • Diabetes Typ II, COPD (paCO2>60mmHg), hypertension, smoker, coronary artery disease, , 90 kg, 170cm, • Lab: Bili 0,8, ASAT 428, ALAT 188, y-GT 140, Quick 60, Crea 3,3 • ultrasound abdomen: Liver steatotic, arteriosclerosis • Questions: • Brain deathimpossibletocertify (paCO2> 60 mmHg = noapnoetest = DCD) • Noorgansuitablefordonation -> tissueonlydonor • Liverandkidney: intra-operative assessment -> thenfurtherdecisions
67 yr., 4 daysagocardiacresuscitation (45 min) • absolute Arrhythmia, norepinehrine, anuria, haemoflitration (4 days) • Diabetes Typ II, COPD (paCO2>60mmHg), hypertension, smoker, coronary artery disease, , 90 kg, 170cm, • Lab: Bili 0,8, ASAT 428, ALAT 188, y-GT 140, Quick 60, Crea 3,3 • ultrasound abdomen: Liver steatotic, arteriosclerosis • Wife: he carried a donorcard • Brain death: cerebralcirculatoryarrest in all 4 vessels (TCD) • -> intraoperatively: Liveryes,Kidneyno(severeArteriosclerosis)- arteriosclerosismightberiskfactorforbiliarytreearteries- still: acutekidneyinjuryis reversible -> Liver recipient: 40 yr. (child B cirrhosis: HBV + HCC), functioning > 2 yr.
55 yr., male, head trauma • Car-crash (side), multiple head fractures & traumatic SAH • Listed for liver transplantation (Hepatitis C, Child A cirrhosis) • anti-HAV-IgG + (IgM -), anti-HEV-IgG + (IgM -) • Hepatitis C genotype 4, non-responder to antiviral therapy • Phone call 21:30 – donor?: • proceed with request to donation and brain death determination? • neurosurgeon: stopped therapy for patient (no brainstem reflexes)! • Questions: • Proceed with donation, Hepatitis C is no contraindication for donation • Proceed with donation, but only the few Hepatitis C-viraemic recipients are eligible as recipient • Stop, multiple Hepatitis infection are a contraindication. • Wait: Child A cirrhosis is not an indication for liver transplantation, information is missing
55 yr., male, head trauma • Car-crash (side), multiple head fractures, traumatic SAH etc. • Listed for liver transplantation (Hepatitis C, Child A cirrhosis) • anti-HAV-IgG + (IgM -), anti-HEV-IgG + (IgM -) • Hepatitis C genotype 4, non-responder to antiviral therapy • heaptocellular carcinoma (HCC) segment 8, MRT-TACE scheduled, chemoembolisation done, CT Abdomen and CT Thorax before LTX!!!!!! • At the phone 21:32 – donor?: • indication for liver transplantation is HCC • Questions: • Proceed with donation, only Hepatitis C-viraemic and extended recipients are eligible. • HCC transmission risk limits use of organs to special cases (plus Hepatitis C problem) • Stop, HCC under therapy is a contra indication • If no metatases are detected in the Thorax-Abdomen CT you may consider EDC-donation
55 yr., male, head trauma • Car-crash (side), multiple head fractures, traumatic SAH etc. • Listed for liver transplantation (Hepatitis C, Child A cirrhosis) • anti-HAV-IgG + (IgM -), anti-HEV-IgG + (IgM -) • Hepatitis C genotype 4, non-responder to antiviral therapy • heaptocellular carcinoma (HCC) segment 8, MRT-TACE, chemoembolisation, CT Abdomen and CT Thorax before LTX!!!!!! • Decision: no donor • the current situation does not exclude metastases even after normal CT. • guidelines: current cancer-therapy = contra indication • LTX is done on the assumption that no metastases exist and therefore immuno-suppression is of no harm (CT before LTX). Then theoretically organs should be free of tumor cells, but true evidence is lacking………
Bloodgroup control: helpful? ten months ago hip operation: 0 Dpos, two transfusion of 0 Dpos 0 cc??ee, Anti-D at control Donor 75 yr., Intracranial beeding (phenprocumon, minor trauma) • Questions: • Impossible, somethinggotmixedup! • Rhesus anti-D andbloodgroupdeterminationtroubleexcludesdonation ! • Rhesus is not consideredin transplantation -> unimportant ! • Gene defectwithoutharmtoorgans, but considerimmunologicalpitfalls !
Bloodgroup control: helpful? ten months ago hip operation: 0 Dpos, two transfusion of 0 Dpos 0 cc??ee, Anti-D - transfusions 0 ccddee - pitfall in blood grouping - check everything for correctness, bedside test helpful too RHD-gene Dpartial 0 cc Dpa ee (DHAR RH33) - expressed on erythrocyte* - counseling for offspring Donor 75 yr., Intracranial beeding (phenprocumon, minor trauma) *passenger lymphocyte -> haemolysis in recipient