Download
1 / 2
20 likes | 194 Views
The author operated 1500 hernias ( 2001-2010). Using for the 1200 first hernias a regular flat mesh or a lightweight mesh . The 300 first hernias have been analysed (2001-2004) (2) The mean follow -up time was 18 months. The rate of follow up was 85%.

E N D
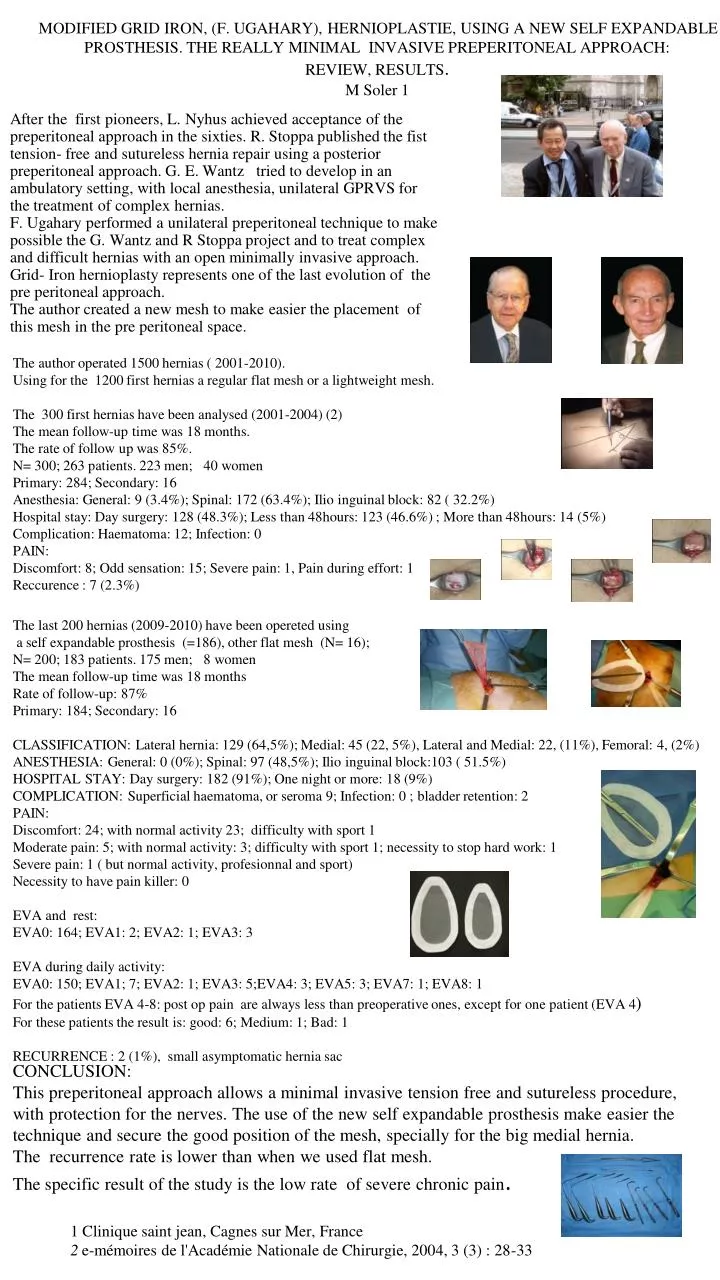
The authoroperated 1500 hernias ( 2001-2010). Using for the 1200 first hernias a regular flat mesh or a lightweightmesh. The 300 first hernias have been analysed (2001-2004) (2) The meanfollow-up time was 18 months. The rate of follow up was 85%. N= 300; 263 patients. 223 men; 40 women Primary: 284; Secondary: 16 Anesthesia: General: 9 (3.4%); Spinal: 172 (63.4%); Ilio inguinal block: 82 ( 32.2%) Hospitalstay: Day surgery: 128 (48.3%); Lessthan 48hours: 123 (46.6%) ; More than 48hours: 14 (5%) Complication: Haematoma: 12; Infection: 0 PAIN: Discomfort: 8; Odd sensation: 15; Severe pain: 1, Pain during effort: 1 Reccurence : 7 (2.3%) MODIFIED GRID IRON, (F. UGAHARY), HERNIOPLASTIE, USING A NEW SELF EXPANDABLE PROSTHESIS. THE REALLY MINIMAL INVASIVE PREPERITONEAL APPROACH: REVIEW, RESULTS.M Soler 1 The last 200 hernias (2009-2010) have been operetedusing a self expandableprosthesis (=186), other flat mesh (N= 16); N= 200; 183 patients. 175 men; 8 women The meanfollow-up time was 18 months Rate of follow-up: 87% Primary: 184; Secondary: 16 CLASSIFICATION: Lateralhernia: 129 (64,5%); Medial: 45 (22, 5%), Lateral and Medial: 22, (11%), Femoral: 4, (2%) ANESTHESIA: General: 0 (0%); Spinal: 97 (48,5%); Ilio inguinal block:103 ( 51.5%) HOSPITAL STAY: Day surgery: 182 (91%); One night or more: 18 (9%) COMPLICATION: Superficialhaematoma, or seroma 9; Infection: 0 ; bladderretention: 2 PAIN: Discomfort: 24; with normal activity 23; difficultywith sport 1 Moderate pain: 5; with normal activity: 3; difficultywith sport 1; necessity to stop hard work: 1 Severe pain: 1 ( but normal activity, profesionnal and sport) Necessity to have pain killer: 0 EVA and rest: EVA0: 164; EVA1: 2; EVA2: 1; EVA3: 3 EVA duringdailyactivity: EVA0: 150; EVA1; 7; EVA2: 1; EVA3: 5;EVA4: 3; EVA5: 3; EVA7: 1; EVA8: 1 For the patients EVA 4-8: post op pain are alwayslessthanpreoperativeones, except for one patient (EVA 4) For these patients the resultis: good: 6; Medium: 1; Bad: 1 RECURRENCE : 2 (1%), smallasymptomatichernia sac After the first pioneers, L. Nyhus achieved acceptance of the preperitoneal approach in the sixties. R. Stoppa published the fist tension- free and sutureless hernia repair using a posterior preperitoneal approach. G. E. Wantz tried to develop in an ambulatory setting, with local anesthesia, unilateral GPRVS for the treatment of complex hernias. F. Ugahary performed a unilateral preperitoneal technique to make possible the G. Wantz and R Stoppa project and to treat complex and difficult hernias with an open minimally invasive approach. Grid- Iron hernioplasty represents one of the last evolution of the pre peritoneal approach. The author created a new mesh to make easier the placement of this mesh in the pre peritoneal space. CONCLUSION: This preperitoneal approach allows a minimal invasive tension free and sutureless procedure, with protection for the nerves. The use of the new self expandable prosthesis make easier the technique and secure the good position of the mesh, specially for the big medial hernia. The recurrence rate is lower than when we used flat mesh. The specific result of the study is the low rate of severe chronic pain. 1 Clinique saint jean, Cagnes sur Mer, France 2e-mémoires de l'Académie Nationale de Chirurgie, 2004, 3 (3) : 28-33