Download
1 / 31
310 likes | 529 Views
Severe Acute Respiratory Syndrome (SARS) Overview and Response Priorities. Jeffrey S. Duchin, M.D . Chief, Communicable Disease Control, Epidemiology and Immunization Section, Public Health - Seattle & King County Division of Allergy and Infectious Diseases, University of Washington.

E N D
Severe Acute Respiratory Syndrome (SARS) Overview and Response Priorities Jeffrey S. Duchin, M.D.Chief, Communicable Disease Control, Epidemiology and Immunization Section, Public Health - Seattle & King County Division of Allergy and Infectious Diseases, University of Washington
Severe Acute Respiratory Syndrome Chronology • SEPT 2003: 8098 cases (774 deaths) reported from 29 countries; 10% case fatality rate, range 0 to >50% Country Cases Deaths China 5327 349 Hong Kong 1755 299 Taiwan 346 37 Canada 251 43 Singapore 238 33 Viet Nam 63 5 USA 29 0
Severe Acute Respiratory Syndrome U.S. Cases Through 15 July, 2003
Severe Acute Respiratory SyndromeBackground • It is not known if SARS will recur, but it is important to be prepared for that possibility • SARS disproportionately affected hospital staff compounding its impact on the health care system • Hospitals served as settings for amplification of transmission leading to community spread • Hospital and community-based infection control measures are the most important way to interrupt SARS transmission • “SARS preparedness” is applicable to a broad range of public health emergencies
Severe Acute Respiratory SyndromeChallenges • No “rapid test” available to diagnose SARS • No specific treatment • No vaccine • Potential large scale public health emergency/disaster • resource implications • logistical challenges • impact on health care delivery system • Communication • Disease containment: Potential need for mandatory and/or large-scale isolation and quarantine measures
Severe Acute Respiratory Syndrome2002-3 SARS Cases and Investigations • Approximately 140 investigations of possible SARS cases (beginning mid-March) • 18 of the 140 classified as suspect SARS cases (no pneumonia) • Over 156 contact investigations related to suspect SARS cases • One suspect SARS case in a health care worker exposed to a suspect SARS patient
Severe Acute Respiratory Syndrome Surveillance • Surveillance is the foundation for SARS control activities • Rapid identification of cases and close contacts is necessary to prevent transmission • Dependant on health care providers and hospitals to promptly identify & report cases meeting current screening criteria • Clinical and epidemiological (exposure) components • Emphasis on identifying exposures in health care settings
Severe Acute Respiratory Syndrome Surveillance • Screening criteria and clinical management recommendations will be “dynamic” and modified to correspond to the level of SARS activity in the world and locally • The key to recognizing persons with SARS is the exposure history - identifying a link to another cases of SARS or a setting where SARS-CoV transmission is occurring
Severe Acute Respiratory Syndrome Surveillance in the Absence of SARS Activity Worldwide • At this time, SARS should only be considered in patients who: • Are hospitalized for pneumonia of unknown etiology AND • Have evidence of one of the following within 10 days of symptom onset: • recent travel to mainland China, Hong Kong, or Taiwan • employment as a healthcare worker with direct patient contact • part of a cluster of unexplained atypical pneumonia cases
Severe Acute Respiratory Syndrome Surveillance in the Presence of SARS Activity Worldwide • Updated screening criteria will be provided to identify persons with fever or cough and relevant SARS exposure history in the 10 days before onset of symptoms
Severe Acute Respiratory Syndrome Washington Administrative Code (WAC) 246-101 Notifiable Conditions Reporting • Who is required to report: • Principal health care providers, and other physicians in attendance are required to report notifiable conditions unless notification has already been made • Health care facilities
Severe Acute Respiratory Syndrome Washington Administrative Code (WAC) 246-101 Notifiable Condition Reporting Requirements • Cooperate with public health authorities during investigations of cases and suspected cases of notifiable diseases • Provide adequate and understandable instruction in disease control measures to each patient who has been diagnosed with a communicable disease and to contacts who may have been exposed the disease
Severe Acute Respiratory SyndromeSARS Investigation Steps • Screen reports of pneumonia and febrile respiratory illness using SARS surveillance criteria • Interview the patient, health care workers • Review medical records • Request isolation of persons suspected to have SARS • Monitor cases under voluntary isolation until 10 days after resolution of fever and respiratory symptoms
Severe Acute Respiratory SyndromeSARS Investigation Steps: Contact Management • Interview patients who meet screening criteria and their contacts, including health care workers, to identify close contacts potentially at risk for SARS • Monitor close contacts (healthcare workers, household members, co-workers, traveling companions, etc) • follow-up SARS investigation and disease control measures if symptoms develop • Recommend appropriate isolation, infection control measures, lab testing and follow-up for cases and exposed persons • Determine case classification, report to state and CDC • Ensure submission of appropriate laboratory tests, track results
Severe Acute Respiratory Syndrome SARS Investigation Steps: Contact Management • Current CDC guidance: In the absence of fever or respiratory symptoms, close contacts of SARS patients need not limit their activities outside the home. • Potential role for quarantine of asymptomatic contacts? • Used extensively in other countries last season
Severe Acute Respiratory SyndromeSARS Investigation Steps: Contact Management • Health care workers (and others) with exposures to suspected SARS cases should be be monitored for 10 days for respiratory symptoms and fever • Health care workers with unprotected high-risk exposures to SARS patients should be excluded from duty for 10 days • Defined as present in the room of a SARS patient during a high-risk aerosol-generating procedure or event and where recommended infection control precautions were absent or breached
Severe Acute Respiratory SyndromeSARS Case Definition: Epidemiological Criteria • Close contact is defined as having cared for or lived with a person known to have SARS, or having a high likelihood of direct contact with respiratory secretions and/or body fluids of a patient known to have SARS. • Examples of close contact include kissing or embracing, sharing eating or drinking utensils, close conversation (<3 feet), physical examination, and any other direct physical contact between persons. • Close contact does not include such activities such as walking by a person or sitting across a waiting room or office for a brief period of time.
Severe Acute Respiratory SyndromeTransmission and Infection Control
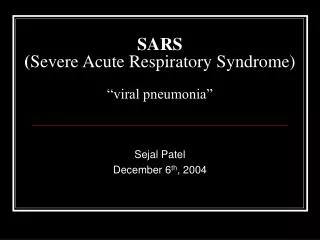
Total SARS Cases and Proportion of Cases Among Healthcare Workers by Country Total No. SARS cases % HCW
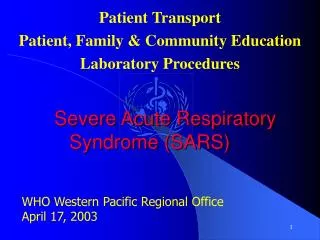
Severe Acute Respiratory SyndromeTransmission: Superspreaders, Singapore 172 Probable SARS Cases by reported source of infection FEB 25 - APR 30, 2003 Source: MMWR May 9, 2003 / 52(18);405-411
Severe Acute Respiratory SyndromeTransmission • Spreads primarily to close contacts by direct contact • Respiratory droplets and secretions • Other infectious body fluids, secretions, and substances • Indirect contact: contaminated objects/environment • Hand hygiene and attention to contact transmission is critical • Possible airborne transmission • To date, no evidence to suggest that SARS is transmitted from asymptomatic individuals
Severe Acute Respiratory SyndromeInfection Control in the Presence of SARS Activity - Isolation • Persons with SARS exposure and pneumonia or ARDS and no alternative diagnosis are to remain under SARS isolation precautions and adhere to infection control recommendations until 10 days after fever resolves and respiratory symptoms improving
Severe Acute Respiratory SyndromeInfection Control in the Presence of SARS Activity - Isolation • Persons with SARS exposure and fever or respiratory symptoms should remain under SARS isolation precautions and adhere to infection control recommendations for a minimum of 72 hours • If symptoms resolve, no restrictions • If symptoms persist but still do not progress to pneumonia, additional 72-hour isolation followed by re-evaluation • If progress to pneumonia and no alternative diagnosis, isolation until 10 days after fever resolves and respiratory symptoms improving
Severe Acute Respiratory SyndromeCDC Household Isolation Guidelines • SARS patients should limit interactions outside the home and should not go to work, school, out-of-home child care, or other public areas until 10 days after the resolution of fever, provided respiratory symptoms are absent or improving • During this time, infection control precautions should be used to minimize the potential for transmission. • In the absence of fever or respiratory symptoms, household members or other close contacts of SARS patients need not limit their activities outside the home.
Draft-Algorithm to Work Up and Isolate Symptomatic Persons who may have been Exposed to SARS Fever or Respiratory Illness1 in Adults Who May Have Been Exposed to SARS Begin SARS isolation precautions, initiate preliminary work-up; notify Health Department2 - CXR No Radiographic Evidence of Pneumonia Alternative diagnosis confirmed3 No Alternative Diagnosis Consider D/C SARS isolation precautions5 Continue SARS isolation and re-evaluate 72 hours after initial evaluation Symptoms improve or resolve Persistent fever or unresolving respiratory symptoms Perform SARS test; continue SARS isolation for additional 72 hr. At end of the 72 hrs, repeat clinical evaluation including CXR + CXR No radiogrpahic evidence of pneumonia Consider D/C SARS isolation precautions5 Use algorithm for CXR + cases
Using Alternative Diagnosis to Rule Out” SARS Based on test with high positive predictive value Clinical course consistent No evidence of clustering No strong epidemiologic link Algorithm to Work Up & Isolate Symptomatic Persons who may have been Exposed to SARS Fever or Respiratory Illness1 in Adults Who May Have Been Exposed to SARS Begin SARS isolation precautions, initiate preliminary work-up; notify Health Department2 Radiographic Evidence of Pneumonia Perform SARS testing Laboratory evidence of SARS-CoV or No alternative diagnosis Alternative diagnosis confirmed Consider D/C SARS isolation precautions Continue SARS isolation until 10 days following resolution of fever given respiratory symptoms are absent or resolving
Severe Acute Respiratory SyndromeInfection Control - Disposition • Patients should not be hospitalized solely for the purpose of infection control/isolation unless they cannot be discharged directly to their home (e.g. travelers, homeless persons) or if infection control precautions recommended for the home or residential setting are not feasible in their home environment
Severe Acute Respiratory SyndromeIsolation and Quarantine: Process • Rely on patients to comply with voluntary isolation request • Requires access at site of care to current versions of official isolation requests, printed instructions and guidelines, Q & A, etc., for patients and exposed persons • Critical importance of patient education by health care workers regarding need for compliance with isolation and with infection control recommendations • Mandatory isolation order is possible if voluntary isolation fails • Requires specific procedures and documentation
Severe Acute Respiratory SyndromeCDC Guidelines: Community SARS Preparedness • Supplement A: Command and control • Supplement B: SARS surveillance • Supplement C: Preparedness and response in healthcare facilities • Supplement D: Community containment measures • Supplement E: Managing travel associated risk • Supplement F: Laboratory diagnosis • Supplement G: Communication