Download
1 / 30
300 likes | 470 Views
Evidence. TERESA BERNARD GIBSON, PHD SENIOR DIRECTOR, HEALTH OUTCOMES NOVEMBER 16, 2011. OVERVIEW. Background Evaluating Effects Evidence 2 Studies Evidence in Progress Desirable Evidence. EVIDENCE.

E N D
Evidence TERESA BERNARD GIBSON, PHD SENIOR DIRECTOR, HEALTH OUTCOMES NOVEMBER 16, 2011
OVERVIEW Background Evaluating Effects Evidence 2 Studies Evidence in Progress Desirable Evidence
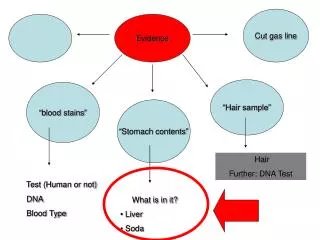
EVIDENCE • Probability of a commercial airline flight with a physician-passenger: 0.7 (range: 0.5-0.85) • Groeneveld et al. JAMA. 2001. 286(12): 1482-1489.
RAND HEALTH INSURANCE EXPERIMENT Manning et al. Health Insurance and the Demand for Medical Care. 1988. Santa Monica, CA : The Rand Corporation. • Design • 6 Cities: Seattle, WA; Dayton, OH; Charleston, SC: Fitchburg-Leominster, MA; Franklin County, MA; Georgetown County, SC • Fee-for-Service Plans: • Free (0% coinsurance) • 25% coinsurance • 50% coinsurance • 95% coinsurance • Outpatient individual deductible • Maximum Dollar Expenditure per year • 5, 10 or 15 percent of income • No more than $1000 (average income was around $10K)
RAND HEALTH INSURANCE EXPERIMENT • No selection of health plan • Assigned to health plan • Balanced characteristics of groups assigned to health plan options • Random sample from cities • Findings • “The data from the HIE clearly show that the use of medical services responds to changes in the amount paid out of pocket.” p. ix.
EVALUATING EFFECTS • How do we know that an intervention works? • What are the effects of an intervention? • How does an intervention perform in a real-world setting?
THE EVIDENCE • Strength/Intensity of the Intervention • Include brand and/or generic medications • Amount of reduction in cost-sharing • Percentage reduction in cost-sharing • Qualification for reduction in cost-sharing • Disease-specific, medication-specific, incentive for engagement? • Comparison group • Internal/external • Assignment to intervention/comparison group • Randomization, matching • Length of time studied
THE EVIDENCE • Size of groups • Outcomes/Measures • Methods of Comparison • Falsification tests • Effects of the program on outcomes not related to the program
THE EVIDENCE • Design elements • Context • VBID programs in place • Other programs in effect • An individual’s previous program • From To
Gibson and Colleagues Health Affairs 2011; 30(1): 100-108. • Strength/Intensity of the Intervention • 3 Tier 10%/20%/35% 1 Tier 10% • Diabetes • Comparison group • Internal (same firm) • Selected sites received the VBID, other sites did not • One-to-one propensity score matching • VBID + Disease Management Disease Management • VBID/No Disease Management No Disease Management • Also matched Disease Management to similar employers in the MarketScan Database
Gibson and Colleagues Health Affairs 2011; 30(1): 100-108. • Length of time studied • 3 years post-implementation • Size of groups • VBID + Disease Management: 1,876 • VBID, no Disease Management: 328 • Outcomes/Measures • Adherence/Medication Utilization • Receipt of Guideline-related Utilization • Spending • Methods of Comparison • Multivariate models, panel data framework
RESULTS • The combination of VBID and disease management is more powerful than disease management alone: all effects higher • Prescription drug utilization • All antidiabetic medications • Oral antidiabetic medications • Insulin • Brand/generic antidiabetic medications • Adherence to recommended medical service guidelines • PCP Visits, HbA1c tests, Urinalysis, Lipid tests • Retinal eye exams unaffected • Patients may have been using vision care benefits (not medical benefits) to receive eye exams
RESULTS: VBID WITHOUT DISEASE MANAGEMENT • The effects on those who opted out of a diabetes disease management program (VBID with no disease management compared to no disease management) resulted in higher levels of adherence to a 0.8 MPR threshold or higher, but no other lasting effects among other measures. • Among those who opted out, the sample size was smaller (n=328), which may have reduced statistical power • The majority were enrolled in an HMO (tighter medical management)
RESULTS: SPENDING • VBID and disease management group • All-cause • Prescription drug spending • Medical spending: • Total (medical plus drug spending): • Diabetes-related • Prescription drug spending: • Medical spending: • Total spending: • Spending effects for the VBID group without disease management:
Choudhry and Colleagues NEJM; online first November 14, 2011. • MI FREEE Trial • Post Myocardial Infarction Free Rx Event and Economic Evaluation (MI FREEE) Trial • Strength/Intensity of the Intervention • Existing Plan $0 copayment for statins, beta blockers and ACEI/ARB • Patients post-Acute Myocardial Infarction hospitalization • Comparison group • Cluster randomized by plan sponsor (e.g., employer, union) within a large insurer randomized to full coverage or existing plan prior to intervention • Plan sponsors agreed to participate or not
Choudhry and Colleagues NEJM; online first November 14, 2011. • Length of time studied • Varied, median 294 days (IQR: 201-663 days) • Size of groups • Full coverage (2,845 patients, 1,494 plan sponsors) • Usual coverage (3,010 patients, 1,486 plan sponsors) • Outcomes/Measures • Medication Utilization • Percent of days covered, Percent fully adherent • Clinical • First major vascular event or revascularization, total vascular events and revascularization, first major vascular event • Spending
RESULTS (FULLY COVERED VS. USUAL COVERAGE) • Adherence/Medication Utilization • Percent of days covered for all classes (ACEI/ARB, beta blockers, statins, all classes) • Percent of patients that were fully adherent for all medication classes • Clinical Outcomes • First major vascular event or revascularization • Major vascular events (fatal or nonfatal MI, stable angina, CHF, stroke): • Total major vascular events or revascularization:
RESULTS • Effects on Health Spending • Patient Spending (out of pocket): • Prescription drug: • Medical: • Total: • Total Spending (health plan, patient): • Prescription drug: • Medical: • Total:
EVIDENCE IN PROGRESS • Incentive-based wellness programs • Biometric screenings, counseling to interpret results • Health Risk Appraisal • Incentive platform to improve health and manage health • VBID component for condition(s) • Prescription drugs • Supplies • Office visits
DESIRABLE EVIDENCE • Role of office visit cost-sharing • Brand and generic medications • Substitutes and/or complements • Income and use of brand and generic medications • Cost-sharing and children • Cost-sharing and productivity • Cost-sharing and mortality • Pilote et al. 2002 (no effect), Choudhry et al. 2011 (death rates from cardiovascular causes lower in intervention group) • After Acute Myocardial Infarction
DESIRABLE EVIDENCE • Optimal health insurance • Balance moral hazard with risk aversion • Randomization to intervention/control groups • Effects of combining incentives and programmatic elements • Incentive-based wellness programs
REFERENCES Chang A, Liberman JA, Coulen C, Berger JE, Brennan TA. Value-based insurance design and antidiabetic medication adherence. Am J Pharm Benefits 2010; 2(1): 39-44. Chernew ME, Shah MR, Wegh A, et al. Impact of decreasing copayments on medication adherence within a disease management environment. Health Affairs 2008; 27(1): 103-112. Choudhry NK, Fischer MA, Avorn J, et al. At Pitney Bowes, value-based insurance design cut copayments and increased drug adherence. Health Affairs 2010; 29(11): 1995-2001. Choudhry NK, Avorn J, Glynn RJ, et al. Full coverage for preventive medications after myocardial infarction. NEJM 2011; online first. Gibson TB, Wang S, Kelly E, et al. A value-based insurance design program at a large company boosted medication adherence for employees with chronic illnesses. Health Affairs 2011a; 30(1): 109-117. Gibson TB, Mahoney J, Ranghell K, Cherney BJ, McElwee N. Value-based insurance plus disease management increased medication use and produced savings. Health Affairs 2011b; 30(1): 100-108.
REFERENCES Kim YA, et al. Evaluation of Value-Based Insurance Design with a Large Retail Employer. AJMC 2011; 17(10): 682-690. Maciejewski ML, Farley JF, Parker J, Wansink D. Copayment reductions generate greater medication adherence in targeted patients. Health Affairs 2010; 29(11): 2002-2008. Zeng F, An JJ, Scully R, Barrington C, Patel BV, Nichol MB. The impact of value-based benefit design on adherence to diabetes medications: A propensity score-weighted difference in difference evaluation. Value in Health 2010; 13(6): 846-852.