Download
1 / 39
410 likes | 647 Views
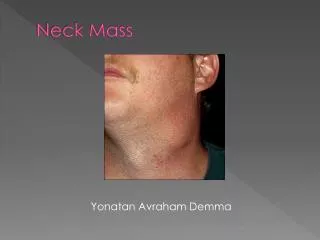
Evaluation and Management of the Patient with a Neck Mass. Bastaninejad , Shahin , MD, ORL and HNS Specialist. Anatomy. History and P.Exam . Historical Points. Age: Up to 15yrs (pediatrics) more than 90% benign 16 to 40 (young adult)

E N D
Evaluation and Management of the Patient with a Neck Mass Bastaninejad, Shahin, MD, ORL and HNS Specialist
Historical Points • Age: • Up to 15yrs (pediatrics) more than 90% benign • 16 to 40 (young adult) • More than 40yrs (older adults) 80% neoplasm 80% of them malignant (secondary>>primary) • Time course • immunodeficiency
Prior trauma • Travel, Irradiation, Surgery • Associated symptoms fever, dysphagia, weight loss, otalgia, hearing loss, respiratory difficulties • Perform a FULL head and neck examination
FNA if unsuccessful or less informative consider Re-FNA failure again consider core needle Bx Failure again excisionalBx and if it was SCC, consider simultaneous neck dissection procedure
Inflammatory causes • The most common neck masses • LAP: • typically subside without tx • sometimes it become necrotic and an abscess forms (Staph./Strep.) • Granulomatous disease: TB, atypical mycobac., actinomycosis, cat scratch, syphilis. • FNA better than excision (because of the risk of non-healing wound)
Sialadenitis and Sialolithiasis • Abx • Hydration • Warm compresses • Massage • sialogogues
Congenital neck masses • TGDC • In pediatric they are second in frequency only to LAP • Elevates in the neck with tongue protrusion • If it becomes infected: Avoid I&D Choice is Aspiration and Abx. • Main procedure is Sistrunk procedure
Branchial cleft anomalies • Anomalies: cyst, sinus, fistula • 30% of the pediatric neck masses • 95% of them 2nd Arch anomaly: • Manifest as a lateral neck swelling associated with an URI • Like TGDC, avoid I&D • Tract pathway is lateral to the ICA, and enters to the pharynx at the tonsillarfossa • Its swelling bulk or draining tract is anterior to the SCM muscle
1stBranchialCleft anomaly • 1% of branchial cleft anomalies • Associated with VII nerve • Fistula, cyst & sinuses located between EAC and the angle of the mandible • Type 1: EAC duplication, contain ectodermal elements, it’s lateral to the VII nerve • Type 2: Contain ectodermal and mesodermal elements (mesocartilage), it’s deep to the VII nerve
3rd and 4th BCA • Extremly uncommon • Swelling or sinus tract in the lower neck, anterior to the SCM muscle • 3rd: Deep to the CA, pierce thyrohyoid membrane and enters the pharynx at pyriform sinus • 4th: Deep to the CA, close to the thyroid gland, enters pyriform sinus or cervical esophagus
Dermoid cyst: contains ectodermal and endodermal elements • Teratomas: • all three germ layers • Less than 2% of all body teratomas are in H&N, most commonly: neck and nasopharynx • Lymphangioma most common in posterior triangle
Hemangioma: • Commonly occure in H&N and it’s present at birth • Phases: • Rapid expansion (6-12mo) • Stable phase; no/minimal change occures • Involution; usually begins by 24mo • 50% complete in 5yr age • Nearly all tumors regress by 10-12yr s age
Primary neoplasm of the neck • Lymphoma: • Most common H&N malignancy in Ped. • 2nd most common overall H&N malignancy second only to SCC (SCC is the most common H&N cancer) • Non Hodgkin (*5) > Hodgkin • 90% B cell
Thyroid neoplasm: • Most common neoplastic anterior neck masses in all age groups • More than 90% of all thyroid nodules are benign • Malignancy probability is greater in very young children, very old age population and males • Salivary gland neoplasm • 1% of all H&N masses • MEC is the most common salivary malignancy
Salivary gland neoplasm, Continue: • %80 is from parotid gland %80 benign majority: benign mixed tumor • %15 SMG %50 malignant • %5 S.Lingual & minor glands More than %75 malignant • Neurogenic Neoplasm: • Schwanoma • Is the most common neurogenictumor • Parapharyngeal space is a common location • Neurofibroma • There is a %2-6 risk of malignant degeneration (malignant nerve sheet tumor)
Neurogenic Neoplasm, Continue: • Neuroblastoma, ganglioneuroblastoma, . . . • Neuroma it is a complication of truma, mainly greater auricular nerve • Paraganglioma neuroectodermal origin • Carotid body (angiographyLyre’s sign) • Jugulotympanic region usually not a neck mass • Vagus nerve
Table 116-2 -- Steps in the Workup of an Unknown Primary Squamous Cell Carcinoma of the Neck