Download
1 / 49
490 likes | 697 Views
Lecture 7 Bio3124. Antimicrobial Chemotherapy. Chemotherapeutic agents. Chemical agents used to treat infectious diseases Kill or inhibit the growth of pathogens within the host Antibiotics Natural microbial products/semi synthetic/synthetic. The Development of Chemotherapy.

E N D
Lecture 7Bio3124 Antimicrobial Chemotherapy
Chemotherapeutic agents • Chemical agents used to treat infectious diseases • Kill or inhibit the growth of pathogens within the host • Antibiotics • Natural microbial products/semi synthetic/synthetic
The Development of Chemotherapy • Paul Ehrlich (1904) • Concept of selective toxicity • identified dyes that effectively treated African sleeping sickness • Sahachiro Hato (1910) • working with Ehrlich, identified arsenic compounds (Salvarsan) that effectively treated syphilis • Gerhard Domagk, and Jacques and Therese Trefouel (1935) • discovered sulfonamides and sulfa drugs Paul Ehrlich 1854 – 1915
Penicillium mold kills S.aureus Penicillin • Ernest Duchesne (1896), discovery lost • Alexander Fleming (1928) • observed penicillin activity on a contaminated plate • did not follow up • effectiveness demonstrated by Florey, Chain, and Heatley (1939) • Fleming, Florey and Chain received Nobel Prize in 1945
Later discoveries • Selman Waksman (1944): Streptomycin, an antibiotic active against tuberculosis • Nobel Prize in 1952 for this discovery • by 1953 chloramphenicol, terramycin, neomycin, and tetracycline were isolated
Properties of an antibiotic • Selective toxicity (Paul Ehrlich) • ability of drug to kill or inhibit pathogen with a minimal or no harm to host For a good antibiotic: • Therapeutic dose • drug level required for clinical treatment; should be low • Toxic dose • drug level at which drug becomes too toxic for patient (i.e., produces side effects); should be high • Therapeutic index • ratio of toxic dose to therapeutic dose; should be high
Determining Antimicrobial Activity • expressed in two ways • minimal inhibitory concentration (MIC) • lowest concentration of drug that inhibits the growth of a pathogen • minimal lethal concentration (MLC) or minimal bactericidal concentration (MBC) • lowest concentration of drug that kills a pathogen • two techniques used to determine MIC and MBC
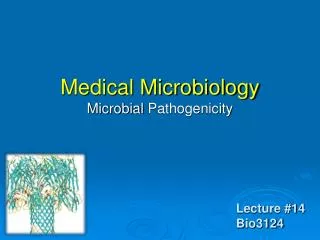
2n 128 64 32 16 8 4 2 0 2n 128 64 32 16 8 4 2 0 MBC=64 ug/ml Antibiotic concentration (ug/ml) Antibiotic concentration (ug/ml) 2n 128 64 32 16 8 4 2 0 Antibiotic free medium Dilution Susceptibility tests • Tube dilution assay:tests for one antibiotic at a time • MIC: half dilution series of AB in Müller Hinton medium prepared • equal amount of bacterial broth added • incubation at 37°C for 18 hours, visible growth checked • MBC: lowest AB concentration to kill completely • Agar dilution assay: a variation of tube dilution assay done on agar containing solid medium where visible colonies are scored (multiple microorganisms vs one type of antibiotic) MIC=16 ug/ml
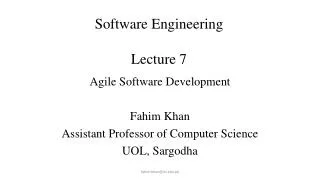
Kirby-Bauer method: disc diffusion test • Agar disc diffusion test:Bacterial culture is uniformly inoculated onto the surface of an agar plate • antibiotic discs are placed onto the plate • antibiotic diffuses out of discs to form a concentration gradient • after incubation the diameter of the zone of growth inhibition is measured and compared to standard tables • the diameter of the zone of inhibition is inversely related to MIC AMP Tb Tet Gm Suceptibility order: Tet>Tb>Gm>Amp
Kirby-Bauer method • standardized method for carrying out disk diffusion test • sensitivity and resistance determined using tables that relate zone diameter to degree of microbial resistance • table values plotted and used to determine if concentration of drug reached in body will be effective
Determining the susceptibility or resistance • MIC values are compared to standard value set by international committees • log2 MIC vs diameter of inhibition zone is linear • effective dosage determined 512 Resistant Intermediate Susceptible 128 64 32 A (μg/ml) 16 8 MIC 4 B 2 0 6 10 14 18 22 Diameter if inhibition zone (mm)
Determining the Therapeutic Dose • antibiotics decay in vivo • time required to keep the serum concentration above MIC • without significant toxicity to host • effective dosage and repetition of dose determined
The E test • similar to disk diffusion method, but uses strip instead of disk • convenient to use, more informative than discs • MIC value can be read directly • E-test strips contain a gradient of an antibiotic • intersection of elliptical zone of inhibition with strip indicates MIC MIC
Classification of antibiotics • inhibitors of cell wall synthesis • β-lactams (penicillins and cephalosporins) • Vancomycin • protein synthesis inhibitors • Aminoglycosides (Kanamycin, Gentamicin etc.) • Tetracyclins • Macrolides • Chloramphenicol • metabolic antagonists • Trimethoprim • Sulfonamides • nucleic acid synthesis inhibitors • Quinolones
1. Inhibitors of Cell Wall Synthesis • Penicillins • 6-aminopenicillanic acid derivatives, differ in side chain • Have b-lactam ring • essential for bioactivity • many penicillin resistant organisms produce b-lactamase (penicillinase) which hydrolyzes a bond in this ring
Mode of action • irreversible competitive binding to the active site of PBPs (transpeptidases), normally catalyse the transpeptidation step in bacterial cell wall synthesis • prevents the synthesis of complete cell walls =>cell lysis • acts only on growing bacteria that are synthesizing new peptidoglycan PBP locked in hemi-acyl reaction on antibiotic PBP catalyzes transpeptidation reaction
Cephalosporins • structurally and functionally similar to penicillins • broad-spectrum antibiotics that can be used on patients that are allergic to penicillin • grouped into four categories based on their spectrum of activity From Cephalosporium acremonium Fourth generation
Resistance mechanisms against B-lactams • Resistance: • PBPs with lowered affinity to β-lactam • Overproduction of β –lactamases • acquisition of inducible β –lactamases • resistance to penicillins, including the semisynthetic analogs, continues to be a problem
Vancomycin • glycopeptide antibiotics produced by Streptomyces orientalis • Competitive binding to terminal D-Ala residues of the peptidoglycan, interferes with transpeptidation reaction of PBPs • vancomycin has been important for treatment of antibiotic resistant staphylococcal and enterococcal infections • considered “drug of last resort” • rise in resistance to vancomycin is of great concern • Resistance: • Mutational change of D-ala-D-Ala to D-Ala-Lactate in cell wall structure
2. Protein Synthesis Inhibitors • many antibiotics bind specifically to the prokaryotic ribosomes • 30S (small) or 50S (large) ribosomal subunits • inhibit a step in protein synthesis • aminoacyl-tRNA binding • peptide bond formation • mRNA reading • Ribosomal translocation • Antibiotics: • Aminoglycosides, Tetracyclines, Macrolides and Chloramphenicol
Aminoglycosides • Wide spectrum, fungal and bacterial metabolic or synthetic products • 1944: first aminoglycoside, Streptomycin from Streptomyces griseus,used to treat of tuberculosis • more synthetic products • Polycationic cyclohexane amino sugars with diverse structural properties • Three families: Kanamycin, Neomycin and Gentamicin • Structural diversity: type of sugar and sugar ring substitutions, ie NH3, OH, H • example shows derivatives in Kanamycin family
Mode of action and resistance mechanism • Mode of action: bind to 16S rRNA of 30S ribosomal subunit and interfere with protein synthesis • ribosomal shifting, amino acid misincorporation, misfolded proteins • Resistance mechanisms:enzymatic modification of ABs that results in loss of capacity to bind the targetModifying enzymes: • Aminoglycosideneucleotidyletransferases (ANTs): covalently bind an NTP in sugar ring I or III • Aminoglycosideacyltransferases (AACs)AAC6’ transfer an acyl group to 6’ position • Aminoglycosidephosphotransferase (APHs): e.g. APH3’ transfers a phosphate group from ATP to the 3’ position
Tetracyclines • produced by Streptomyces or synthesized • are broad spectrum, bacteriostatic, eg. used in acne treatment • all have a four-ring structure to which a variety of side chains are attached • Bind to 30S ribosomal subunit A site • inhibits binding of aminoacyl-tRNA molecules to the A site of the ribosome • Resistance: mutational target modification resulting in loss of binding site
Macrolides • contain 12 to 22-carbon lactone rings linked to one or more sugars • used on patients allergic to penicillin • e.g., erythromycin, Azithromycin • broad spectrum, bacteriostatic • binds to 23S rRNA of 50S ribosomal subunit • inhibits peptide chain elongation • Resistnace:mutationaltarget modification
Chloramphenicol • First isolated from Streptomyces venezuelae • now is chemically synthesized • binds to 23S rRNA in 50S ribosomal subunit and inhibits peptidyl transferase reaction during protein synthesis • Toxic, numerous side effects, carcinogenic • used in life-threatening situations • Resistance:enzymatic acetylation by acetyltransferases on –OH groups
3. Metabolic Antagonists • act as antimetabolites • antagonize metabolic pathways by competitively inhibiting the use of metabolites by key enzymes • are structural analogs • molecules that are structurally similar to, and compete with, naturally occurring metabolic intermediates • Synergism: two antibiotics working together better than individually Dihydrofolic acid analog
Sulfonamides or Sulfa Drugs • structurally related to a p-aminobenzoic acid (PABA) • PABA used for the synthesis of folic acid and is made by many pathogens • unlike humans, these pathogens cannot take up PABA • selectively toxic, compete against PABA for the active site of an enzyme involved in folic acid synthesis, resulting in a decline in folic acid concentration • pathogen dies because folic acid is a precursor to purines and pyrimidines which are nucleic acid building blocks
Trimethoprim • synthetic antibiotic that also interferes with folic acid production • broad spectrum • can be combined with sulfa drugs to increase efficacy of treatment • combination blocks two steps in folic acid pathway • has a variety of side effects including abdominal pain and photosensitivity • Resistance: • Overproduction of PABA • Mutant enzymes that evade the binding of drugs but not the natural substrates
4. Nucleic Acid Synthesis Inhibition • a variety of mechanisms • block DNA replication • inhibition of DNA polymerase • inhibition of DNA helicase • block transcription • inhibition of RNA polymerase • Must target DNA/RNA biosynthetic steps that are different between prokaryotes and eukaryotes
Quinolones • broad-spectrum, synthetic, contain quinolone ring • Nalidixic acid, first synthesized (1962) • Fluoroquinlones like Ciprofloxfacin, norfloxacin are new drugs with a wider antibacterial spectra • act by inhibiting bacterial DNA-gyrase (Topoisomerase II) • disrupts DNA supercoiling and replication • selective toxicity: DNA gyrase is not present in eukaryotic cells • Resistance: • mutations in quinolone binding cleft on gyrase (gyrB subunit) that results in loss of affinity • Reduced uptake due to mutations in ompF gene that encodes for porins • Active efflux pumps
Antifungal Drugs • fewer effective agents because of similarity of fungal cells and human cells • easier to treat superficial mycosis than systemic infections
Antifungal Agents • Fungal infections difficult to treat • Eukaryotic cells similar to animal cells • Fungi inactivate many drugs • Inhibitors: • Treatment of superficial mycosis • Clotrimazole: inhibits sterol synthesis • Griseofulvin: disrupts mitotic spindle formation
Treating systemic infections • Polyene produced by Streptomyces nodosus • binds membrane ergosterol found in fungal membranes • disrupts fungal membrane integrity
Antiviral Drugs • drug development has been slow because it is difficult to specifically target viral cycle • drugs currently used inhibit virus-specific enzymes and life cycle processes
Amantadine • used to prevent influenza infections • Inhibits M2 viral envelop protein • blocks penetration and uncoating of influenza virus
Tamiflu and Zanamivir • anti-influenza agents • neuraminidase inhibitors • prevent the release of virions from infected cells, • not a cure for influenza, has been shown to shorten course of illness A. Oseltamivir (Tamiflu)
inhibits herpes virus enzymes involved in DNA and RNA synthesis and function inhibits herpes virus and cytomegalovirus DNA polymerase inhibits herpes virus DNA polymerase
Anti-HIV drugs • two main targets • HIV reverse transcriptase • HIV protease
Protease inhibitors • Gag polyprotein is expressed from a single mRNA • cleaved by viral protease to viral coat proteins p15, p17and p24 • Ritonavir , inhibitor of protease mimics peptide bond that is normally attacked by the protease
Summary of Mechanisms of Drug Resistance • alteration of target enzyme or organelleeg.PBPs • inactivation of drug • enzymatic modification of drug by pathogen (eg. AGs) • Drug exclusion: prevent entrance of drug • drug can’t bind to or penetrate pathogen • decreased permeability • Efflux pumps: pump drug out • use of alternative pathways or increased production of target metabolite, eg. PABA
Drug Resistance • an increasing problem • resistance mutants arise spontaneously or by mutagen induction and are then selected • once resistance establishes in a population it can be transmitted to other bacteria horizontally by • Transduction: viruses transmit resistance genes • Transformation: genes picked up from environment • Conjugation: conjugative plasmids transmit the resistance genes
After 100 years of golden antibiotic era we have a problem on our hands: Emerging Multidrug Resistance • Multidrug resistance:clinical and social problem inherent to antibiotic era • Reasons? • Mutation rates in bacteria and viruses are enormously high and cumulative • Selection of antibiotic resistant microorganisms is unavoidable direct result of antibiotic use • Increased volume of antibiotic use, most probably prone to improper practice and misuse. Statistical data suggest a direct correlation (see examples..)
Canada, Quebec, Ontario Number of prescriptions per 1000 citizens per year Antibiotics Consumption in Canada
This excess is attributed to What? • 1990 - 300 metric tons of antibiotics were used. • 70% are not used appropriately • Incorrect usage. • Prescription for viral infections. • Prescription for bacterial infections which can recover on their own.
S. pneumoniae resistance to Penicillin and Macrolides in Canada
Economical impact • Bacterial infections and antibacterial resistance constitute an ever increasing problem • this is reflected in leading market share (62%) for anti-bacterial agents • Fast growing antibiotic resistance has negative impact on R&D in pharmaceutical initiatives • the least relative growth in antibacterial sector is alarming
Measures to counter the Acquired Resistance • Public education. • Usages must be effectively controlled. • Eliminate the prophylactic administration in livestock. • Reduce the usage in the household products. • Reduce the prophylactic usage in humans. • Discover and synthesize new antibiotics. • Would this solve the problem? • What are the possible alternatives? • Probiotic approach? • Natural antimicrobial products? Phage therapy? • New antimicrobial targets? Vaccine development?