Download
1 / 5
50 likes | 258 Views
Click to enlarge. Click to enlarge. Click to enlarge. Click to enlarge. Alemtuzumab Infusion-associated Reactions and Management in Multiple Sclerosis. Before Infusion. During Infusion. After Infusion. Lori Mayer, 1 Lise Casady, 2 Gail Clayton, 3 Pedro Oyuela, 4 David H. Margolin 4

E N D
Click to enlarge Click to enlarge Click to enlarge Click to enlarge
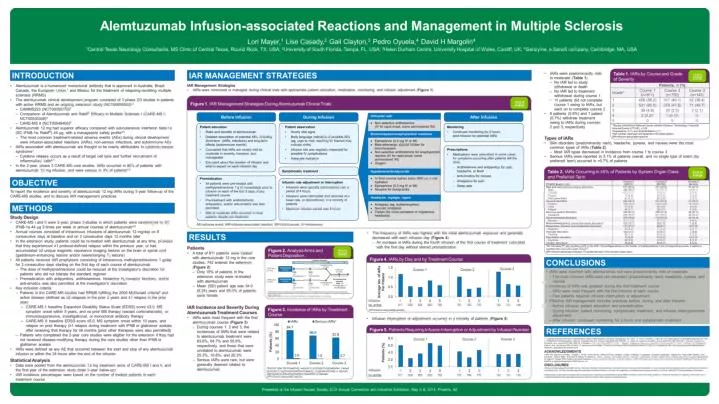
Alemtuzumab Infusion-associated Reactions and Management in Multiple Sclerosis Before Infusion During Infusion After Infusion Lori Mayer,1 Lise Casady,2 Gail Clayton,3 Pedro Oyuela,4 David H. Margolin4 1Central Texas Neurology Consultants, MS Clinic of Central Texas, Round Rock, TX, USA; 2University of South Florida, Tampa, FL, USA; 3Helen Durham Centre, University Hospital of Wales, Cardiff, UK; 4Genzyme, a Sanofi company, Cambridge, MA, USA Figure 1. IAR Management Strategies During Alemtuzumab Clinical Trials • Patient education • Risks and benefits of alemtuzumab • Detailed description of potential AEs, including short-term (IARs, infections) and long-term effects (autoimmune events) • Counseled that IARs are mostly mild-to-moderate in severity, transient, and manageable • Educated about the duration of infusion and what to expect on each infusion day • Patient observation • Hourly vital signs • Body language indicative of possible AEs (eg, urge to void; reaching for blanket may indicate chills) • Infusion site was regularly inspected for possible IV complications • Adequate hydration • Monitoring • Continued monitoring for 2 hours post-infusion for potential IARs • Prescriptions • Medications were prescribed in some cases for symptoms occurring after patients left the clinic: • Antihistamine and antipyretics for rash, headache, or fever • Anti-emetics for nausea • Analgesics for pain • Sleep aids Symptomatic treatment • Premedication • All patients were pre-treated with methylprednisolone 1 g IV immediately prior to infusion on each of the first 3 days of any treatment course • Pre-treatment with antihistamines, antipyretics, and/or anti-emetics was also permitted • Mild or moderate IARs occurred in most patients despite pre-treatment • Infusion rate adjustment or interruption • Infusions were typically administered over a period of 4 hours • Infusions were interrupted and resumed at a lower rate, or discontinued, in a minority of patients • Maximum infusion period was 8 hours AE=adverse event; IAR=infusion-associated reaction; IM=intramuscular; IV=intravenous Back to poster Presented at the Infusion Nurses Society 2014 Annual Convention and Industrial Exhibition, May 3–8, 2014, Phoenix, AZ Presented at the Infusion Nurses Society 2014 Annual Convention and Industrial Exhibition, May 3–8, 2014, Phoenix, AZ