Download
1 / 20
340 likes | 960 Views
Demyelinating Disease. August 27, 2010. Pathologic Criteria. Destruction of myelin Sparing of other elements of the nervous tissue Infiltration of inflammatory cells, prevascularly

E N D
Demyelinating Disease August 27, 2010
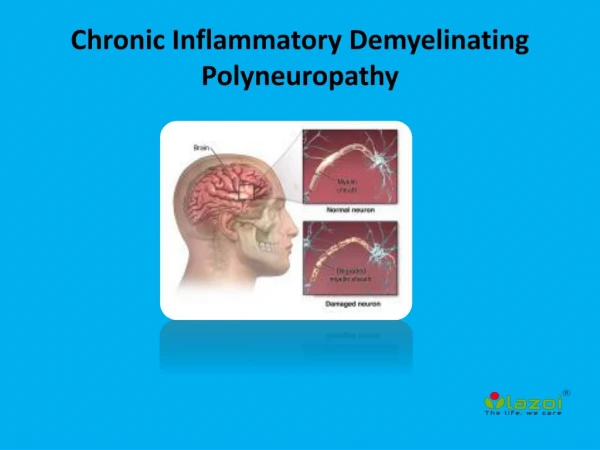
Pathologic Criteria • Destruction of myelin • Sparing of other elements of the nervous tissue • Infiltration of inflammatory cells, prevascularly • Particular distribution of lesions –white matter disease (contains myelinated fiber such as brainstem, thalamus, areas surrounding the ventricles) • Relative lack of Wallerian degeneration or secondary degeneration
Classification of Demyelinating Disease • Multiple sclerosis • Chronic relapsing encephalomyelopathic form • Acute multiple sclerosis • Diffuse cerebral sclerosis Schilder’s and Concentric sclerosis of Balo • Acute disseminated encephalitis • Acute and sub acute necrotizing hemorrhagic encephalitis
Multiple Sclerosis • Disease of young adults • Commonly seen in temperate climates • Subacute disease • Relapses and remissions • Objective evidence of anatomical lesion separated in space and time
Schumacher’s Criteria (1965) • There must be objective abnormalities on neurological examination attributable to dysfunction of the CNS. Symptoms alone, no matter how suggestive, cannot be accepted as diagnostic of MS. • On neurological examination or by history, there must be evidence of involvement of two or more separate parts of the CNS. (Comment: This second criterion is contradictory to the first: symptoms such as diplopia, monocular obscuration of vision, gait ataxia and urinary urgency and incontinence, all classical symptoms of MS, are frequently transient and very often not confirmed by neurological examination. They should not be discarded.) • The objective neurological evidence of CNS disease must reflect predominantly white matter involvement, i.e. fiber tract damage. More than a minor proportion of signs of lower motor neuron (brain stem, spinal nuclear gray matter, or peripheral nerve) dysfunction will disqualify a subject as having MS for purposes of an experimental trial of therapy.
Schumacher’s Criteria (1965) • The involvement of the neuraxis must have occurred temporally in one or the other of the following patterns. • In two or more episodes of worsening, separated by a period of 1 month or more, each episode lasting at least 24 h. • Slow or step-wise progression of signs and symptoms, over a period of at least 6 months. • The ages of the patient at the onset of the disease must fall within the range of 10–50 years inclusive. • The patient's signs and symptoms cannot be explained better by some other disease process, a decision that must be made by a physician competent in clinical neurology.
Frequency of Signs • Spasticity or hyperreflexia or both • (+) Babinski • Absent abdominal reflexes • Impaired position sense • Impaired pain sensation • Incomplete – Check the book!
Frequency of Various Symptoms • Check the book
Course • Exacerbations and remissions • Complete or nearly complete remission chronic • Acute • Rapid progressive – incomplete, check the book • Progressive • Gradual worsening w/o well-delineated remission and relapses • Benign • Few exacerbations (often mild) followed by complete recovery • Subclinical • Demyelination in asymptomatic patients (autopsy)
Some Suggestive Signs/Symptoms • Positive • Combination of pyramidal,cerebellar, posterior column, and brainstem signs • Internuclearopthalmoplegia • Negative • Early development of dementia, seizures or extrapyramidal sign • Noncerebellar tremors, stupor, focal atrophy • Aphasia and fasciculations • Hearing loss and uveitis
Multiple Sclerosis • The cause is unknown and effective treatment has not been identified • Immunologic process is one of the major elements of the disease • Environmental influence, possibly an infectious process, may contribute to the disease • Genetic makeup influences susceptibility to the disease (polygenic)
Treatment • Aimed at halting the progression • Beta-interferon-1a (Avonex) • 31% decrease in exacerbations • 55% incidence of systematic, flu-like symptoms • Given once a month • Beta-interferon-1b (Betasteron) • 34% decrease in exacerbation • Given every other day • 40% will develop antibodies • Glatiramen acetate (Copaxone) • 29% decrease in exacervbations • Given everyday • No significant side effects • Intravenous immunoglobulin (IVIG) • 0.2 gm/kg monthly • Disability scores improved, relapse cut in half • Well-tolerated, few side-effects • Mitoxantrone (Novantrone)
Treatment failure • Severe side effects • 30 or more attacks per year • Steady disease progression • In effective treatments • Hyperbaric oxygen • Long-term use of steroids • Linoleic acid supplementation
Treatment of acute exacerbations • IV methylprednisolone
Demyelinating Disease • Courville et.al. • Acute onset of symptoms affecting young patients predominantly, and proven by autopsy as having CONCENTRIC SCLEROSIS (looks like tree rings/onion layers?)
Baló’s Sclerosis • 33 patients • 6 M • 27 F • Mean age: 28 years • Is monophasic • Infectious in nature • High mortality/survival rate
Clinical Manifestations • Headache • Disturbance in communication • Mental and behavioral changes • Mutism • Fever • Other findings • Disturbance in consciousness
Diagnostic testing • Evoked potentials • Series of electrophysiologic tests that help evaluate the function of specific elements of the Nervous system involve in MS
CSF studies • Normal RBC and glucose • Normal or slightly elevated protein • 5-20 mononuclear cells • IntrathecalIgG synthesis • IncIgG index or 24 hr synthesis rate • Increased Kappa