Download
1 / 33
350 likes | 527 Views
Cerebral Aneurysms in Patients with autosomal dominant Polycystic Kidney Disease (ADPKD) -- Optimal care & Management. Optimal care of autosomal dominant polycystic kidney NEPHROLOGY 2006; 11 , 124–130 Management of Unruptured Cerebral Aneurysms in Patients with Polycystic Kidney

E N D
Cerebral Aneurysms in Patientswith autosomal dominantPolycystic Kidney Disease(ADPKD)-- Optimal care & Management Optimal care of autosomal dominant polycystic kidney NEPHROLOGY 2006; 11, 124–130 Management of Unruptured Cerebral Aneurysms in Patients with Polycystic Kidney Disease Surg Neurol 2004;62:538–45. Present by R2 洪培恩 2007-1-18
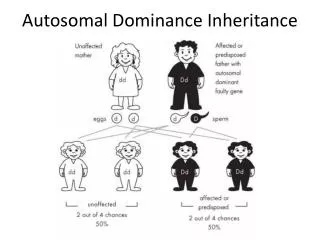
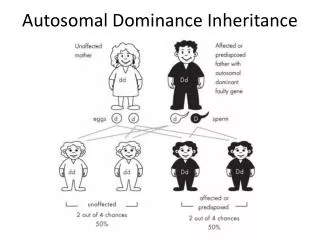
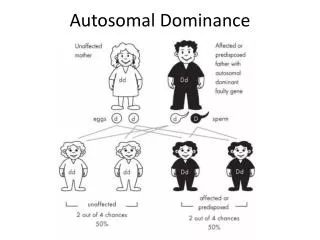
POLYCYSTIC CYSTIC KIDNEY DISEASE ADULT = Autosomal Dominant PKD INFANTILE = Autosomal Recessive PKD Introduction
Epidemiology • Autosomal Dominant Polycystic Kidney Dx • Occurs in approx 1 in 400-1000 population • Only less than 50% of cases are estimated to be diagnosed • One of the most common life-threatening, hereditary disease,10% of all ESRF is ADPKD
Genetic and molecular events • Linked to abnormalities on: Chromosome 16–PKD1 locus (~85%) -- Polycystin-1 protein(a purported receptor for cell–cell or cell-matrix adhesion) Chromosome 4– PKD2 locus(~15%) -- Polycystin-2 protein(appears to be an ion channel, particularly for calcium transport) • Spontaneous Mutation rate 10%
Diagnosis • Frequently asymptomatic • History • Positive family history • Initial Symptoms & Signs • HTN (50-70%; avg 30y/o; renin-angiotension sys) • Flank pain (36%) • Gross hematuria (36%) • Renal infection (16%) • Renal insufficiency • Films • Large kidneys with multiple cysts • Hepatic, Pancreatic, and/or Splenic Cysts • (Hepatic cysts more common in women and pt over 40y/o)
Criteria on Ultrasound • With positive family history • AgeCriteria for Diagnosis <30 >2 cysts uni- or bilateral 30-59 >2 cysts in each kidney >60 >4 cysts in each kidney (-) US cannot exclude disease until 30-35 y/o CT and MRI have higher sensitivity
Extra-renal Complications • Cerebral aneurysms (22%) • Hepatic cysts (83% w/MRI) • Cardiac Valve disease (20-30%) • MV prolapse; MV/AV regurgitation • Colonic diverticula • Abdominal wall & inguinal hernia • Pregnancy • Increased risk of preeclampsia, prematurity and perinatal mortality, ectopic pregnancy with uncontrolled HTN
Risk Factors for Progressive Renal Disease • Younger age at diagnosis • Male sex(European & African-Americans) • Genotype (PKD1 vs PKD2) • (mean age at death: PKD1 53; PKD2 69; control 78) • Episode of gross hematuria • HTN (/c Left Ventricular Hypertrophy) • Proteinuria • Increased/increasing renal size • UTI
Survival data in ADPKDMedian PKD1 = 53yrs Median PKD2 = 69yrs
Relationship between glomerular filtration rate (GFR) and renal volume
Causes of Death • Similar to other causes of ESRD • Heart Disease (36%) • Infection (24%) • Neurologic Event (12%) • Ruptured aneurysm (6%); HTN intracerebral hemorrhage (5%) • Renal Cancer (0%) • Found at Autopsy: • Cardiac Hypertrophy (89%) • CAD (81%)
Increased (a) plasma renin activity (PRA) and (b) plasma aldosterone in autosomal dominant polycystic kidney disease patients (ADPKD) as compared with patients with essential hypertension Activation of the renin-angiotensin-aldosterone system (RAAS)
Multifactorial pathogenic role of angiotensin II in the hypertension and renal disease associated with ADPKD
Treatment • Treatment of choice : ACE Inhibitor • Note use with potential future pregnancy • Efficacy of ARB’s under investigation with limited data available (used as second line) • Goal BP: <120/80 • Screen for occult cerebral aneurysm • S/P if cerebral aneurysm >7-10mm
Correlation between mean arterial pressure and left ventricular mass index (LVMI) in ADPKD
(a)Effect of rigorous versus standard blood pressure control to decrease left ventricular mass index in autosomal dominant polycystic kidney disease (ADPKD) patients. (b) Effect of blood pressure control with amlodipine versus enalapril to decrease left ventricular mass index in ADPKD patients OPTIMAL BLOOD PRESSURE CONTROL v.s LVMI
Treatment • Treatment of progression to ESRD: • Transplantation • With/without nephrectomy • Hemodialysis • (5yr survival: 10-15%)
Experimental animals with ADPKD --slow the progression of the disease • antiproliferative agent,rapamycin • caspase inhibition • and V2 vasopressin antagonists, which decrease renal tissue cyclic adenosine monophosphate(AMP)
Intracranial aneurysm in ADPKD • Occur in 4-11% of patients(general1%) (a defect in the extracellular matrix of the vessels, resulting in a high incidence of cerebral aneurysms) • Tends to run in families • May be worse with hypertension • Tend to suffer their subarachnoid hemorrhage at a younger age and smaller size
Intracranial aneurysm in ADPKD • Most remain asymptomatic • Decision to operate more depends on size, location, age and hypertension, regardless the dialysis status • Screen ‘at risk’ families with MRA, F/U every 10 years if negative J Am Soc Nephrol 15: 1023–1028, 2004
Study for Treatment Strategy • A retrospective review of the management of unruptured cerebral aneurysms in 16 patients with PKD • Considering the potential toxicity of cerebral angiography • 8 p’t maintaining chonic H/D and 8 p’t non-H/D at the time for treatment • F/U period: 24 months
Criteria of prophylactic hemodialysis for Nonhemodialysis patients • moderate to severely reduced renal function (for example, blood urea nitrogen> 80, creatinine> 6, or potassium> 5.5)
In non-H/D p’ts, prophylactic hemodialysis(4 hours)was routinely performed after cerebral angiographyto prevent deterioration of the pre-existing renal dysfunction
Discussion • A prophylactic hemodialysis of 3 to 4 hours can remove 80% of the contrast media • Use gebexate mesylate instead of heparin for post –op hemodialysis to prevent postoperative bleeding from the surgical wounds.
Discussion • Chronic hemodialysis entails specific problems, -Increased intracranial pressure -Progressive brain edema as a result of rapid lowering of the serum osmolality (dialysis disequilibrium syndrome). -Tendency to hemorrhage, in response to either systemic heparinization or insufficient dialysis
Conclusions • Genetic and molecular biology findings have stimulated a great deal of exciting basic research in ADPKD, therapies to decrease morbidity and mortality in ADPKD patients have yet to emerge from these findings • The early diagnosis and treatment of hypertension with inhibitors of the renin-angiotensin-aldosterone system have the potential to decrease or prevent left ventricular hypertrophy cardiac complications and slow the progression of the renal disease.
Conclusions • As patients with PKD live longer because of improved management of their renal dysfunction, the extrarenal manifestations, as exemplified by cerebral aneurysms, may become an even greater problem • PKD patients with unruptured cerebral aneurysms can be safely treated with an appropriate treatment strategy including the use of prophylactic hemodialysis
Others commentary • MRA maybe an excellent way to initially screen these patients, and will often provide sufficient anatomic detail to determine whether intervention is required. • It is often possible to operate on the basis of a MRA, thereby obviating the need for a cerebral angiogram altogether. • If endovascular treatment is subsequently selected, the issues become very important