Download
1 / 24
240 likes | 380 Views
Virginia Survey Process. Medical Director’s role Judy Wilhide Brandt, RN, BA, RAC-MT, C-NE judy@judywilhide.com 909-800-9124 www.judywilhide.com. Basics. Annual survey: Q 9 – 15 months Complaints: PRN Process outlined in SOM Appendix P & PP Very well defined, published survey tasks

E N D
Virginia Survey Process Medical Director’s role Judy Wilhide Brandt, RN, BA, RAC-MT, C-NE judy@judywilhide.com 909-800-9124 www.judywilhide.com
Basics • Annual survey: Q 9 – 15 months • Complaints: PRN • Process outlined in SOM Appendix P & PP • Very well defined, published survey tasks • Structured investigation prescribed by state/federal guidelines • Very subjective decision making/citation assignment
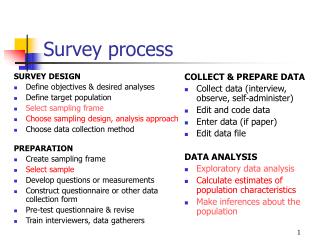
Traditional Survey Process Tasks • Sample Selection- Offsite Survey Preparation: Used to select initial areas of concern & initial residents for sample • ≈60% of residents chosen in Phase 1 & ≈40% in Phase 2 • Quality Measure (QM) Reports • If weight loss, dehydration, and/or pressure ulcerstrigger as a concern, half the phase 1 sample has to have these issues. • Previous survey/complaint history • Waiver/variance info • Ombudsman info • PASSR info
Point: • Areas of concern should never be a total surprise • Discourage “survey prep” mentality just prior to survey window • Encourage IDT to review QMs monthly • Target areas that trigger at 70% to review: • MDS coding • Care concerns • Proper chart documentation to explain whether QM represents an issue or not with appropriate follow up
Quality Measures used in Survey Process Long Stay: • ADL decline • High-risk residents with pressure ulcers • Indwelling catheter • Physically restrained • UTI • Self-report moderate to severe pain • Fall with major injury • Lo Risk Incontinence • Weight Loss • Antipsychotic Use in absence of psychotic/related condition • Depressive Symptoms • Antianxiety/Hypnotic Use • Falls (all) • Behaviors affecting others Short Stay: • New/Worsened Pressure Ulcers • Self-report moderate to severe pain
Comparative Analysis/Benchmarks • Compares your facility to: • Other certified facilities in your state • Other certified facilities nationally • This comparison is used in traditional surveys • Allows you to benchmark your progress and compare yourself to others State Comparison National Comparison/Percentile Ranking You Shall Rise and Show Respect to the Aged
Resident Level Report You Shall Rise and Show Respect to the Aged
Initial Tour • Initial opportunity to observe residents, staff and physical environment including kitchen • Identify residents or potential concerns for investigation • Facility should have staff member who can discuss the resident accompany all surveyors • Very common for most of the worst citations to begin development on the initial tour
Special Considerations for Sample: • Residents: • new admissions • have no or infrequent visitors. • psychosocial, interactive, and/or behavioral needs. • bedfast and totally dependent on care. • dialysis or hospice • Psychotropics • Room variances • MI/DD • Communication issues: Non-oral, languages
Information Gathering • 5A General Observations of the Facility • 5B Kitchen/Food Service Observations • 5C Resident Review • Observation, Interview, Record review • 5D Quality of Life Assessment • 5E Medication Pass and Pharmacy Services • 5F Quality Assessment and Assurance Review • 5G Abuse Prohibition Review
Major Areas Reviewed: • Resident Rights • Admission, transfer, discharge rights • Resident behavior & facility practices • Quality of life • Resident assessment • Quality of care • Nursing services • Dietary services • Physician services • Rehab services • Dental services • Pharmacy services • Infection control • Physical environment • Administration (QA)
Official Top 10 Virginia list 2013 • F-309 Quality of Care • F-514 Clinical records - order • F-280 Care plan 7-days/team/periodic review • F-329 Unnecessary drugs • F-323 Accident prevention - environment • F-502 Laboratory Services • F-278 Accuracy of assessment • F-431 Drugs labels/expired drugs • F=441 Infection Control Program • F-279 Care plan, comprehensive
Most frequent high level citations Virginia 2013 • F-329: Antipsychotics mostly: Need actual behaviors, actual reasons, MD ordering and general statements not sufficient. “dementia with behaviors” certainly not sufficient • F-502: Screwed up labs: Not ordered, not done, not responded to, not done as ordered, not reported, etc. • Diabetic Management: Screwed up with bad outcomes • Injuries: Falls, elopement, physical plant hazards • F441: infection control: Mostly watching med passes, dressing changes, incontinence care, not washing hands by CNAs
Physician Services • F385 Residents’ Care Supervised by Physician • F386 Physician Responsibilities During Visits • F387 Frequency/Timeliness of Physician Visits • F388 Visits by Physician/Phys Assistant/Etc • F389 Emergency Physician Services 24 Hr/Day • F390 Phys Delegation of Tasks in SNFs/NFs
The MedicalDirector • canhelpensurethatappropriatesystemsexist to facilitategoodmedicalcare, • establish and applygood monitoring systems and effectivedocumentation and followup of findings • helpimprovephysiciancompliance with regulations, includingrequiredvisits. • During and after the surveyprocess, the medicaldirectorcan • clarify for the surveyorsclinicalquestionsorinformationabout the care of specificresidents, • requestsurveyorclarification of citations on clinicalcare, • attend the exitconference to demonstratephysicianinterest and help in understanding the nature and scope of the facility'sdeficiencies, • help the facility draft correctiveactions.
Care coordination • A medical director should establish a framework for physician participation, and physicians should believe that they are accountable for their actions and their care. • Ensure primary attending and backup physician coverage; • Ensure that physician/NPP are available to help residents attain and maintain their highest practicable level of functioning, consistent with regulatory requirements; • Develop a process to review basic MD/NPP credentials (e.g., licensure and pertinent background); • Address and resolve concerns and issues between the physicians, health care practitioners and facility staff • Resolve issues related to continuity of care and transfer of medical information between the facility and other care settings.
Common NF Issues in poor survey outcomes • Lack of clinical education by clinical management • Lack of on-going educational development of CNAs, LPNs, RNs, therapists • Perceived or real inadequate staffing • Lack of a robust activities department • Lack of leadership experience/knowledge by administrator/nursing management • Budgetary decisions that do not support quality of care/life
How you can help • Lead the team • Do comprehensive assessments, document legibly your conclusions and plan, every time • Tips: • Diagnose, describe and stage pressure ulcers (yourself) • Diagnose, describe other types of wounds • Avoid simply listing diagnoses without current status and plan • Follow up on resident injuries: Demand careful review by IDT of falls, fractures, etc. • Follow up on infections, changes of condition: Did staff properly recognize and report? Do they know what they are doing clinically? • Prescribe psychotropics when needed and document justification. • Don’t prescribe when not indicated
How you can help • Demand quality of care • Sanitation, hygiene, nutritious, delicious meals • Do you ever eat the food? How about the pureed food? • Restorative nursing • Skin • Dental • Foot care • Demand continuity of care • Shift to shift • Across transitions: Hospital, home health • Pain control • During high risk times: • Newly admitted: Does the staff know how to assess a new resident? Skin, pain, preferences, functional status (falls)
How you can help • Demand appropriate staffing for acuity • Actively engage in QA efforts • Realize that a little pain for the IDT during a survey may result in lasting improvements • Don’t buckle to pressure in survey to ‘write something to make it better’ • Admit your shortcomings, demand the IDT admit theirs: make it better (QAPI) • Stay the course • Tell the truth
Plan of correction: • Be actively involved in survey • Attend exit conference • Assist in implementing realistic POC for lasting change • Root cause analysis • Develop/educate staff • CNA, LPN, RN • Dietary • OT, ST, PT