Download
1 / 2
20 likes | 132 Views
Funded by the MRC. AUTOLOGOUS CHONDROCYTE TRANSPLANTATION/IMPLANTATION VERSUS EXISTING TREATMENTS ISCRCTN 48911177. NEWSLETTER September 2007 Issue 13. Recruitment It’s good to see more centres have got started (Hillingdon, Weston-s-Mare &

E N D
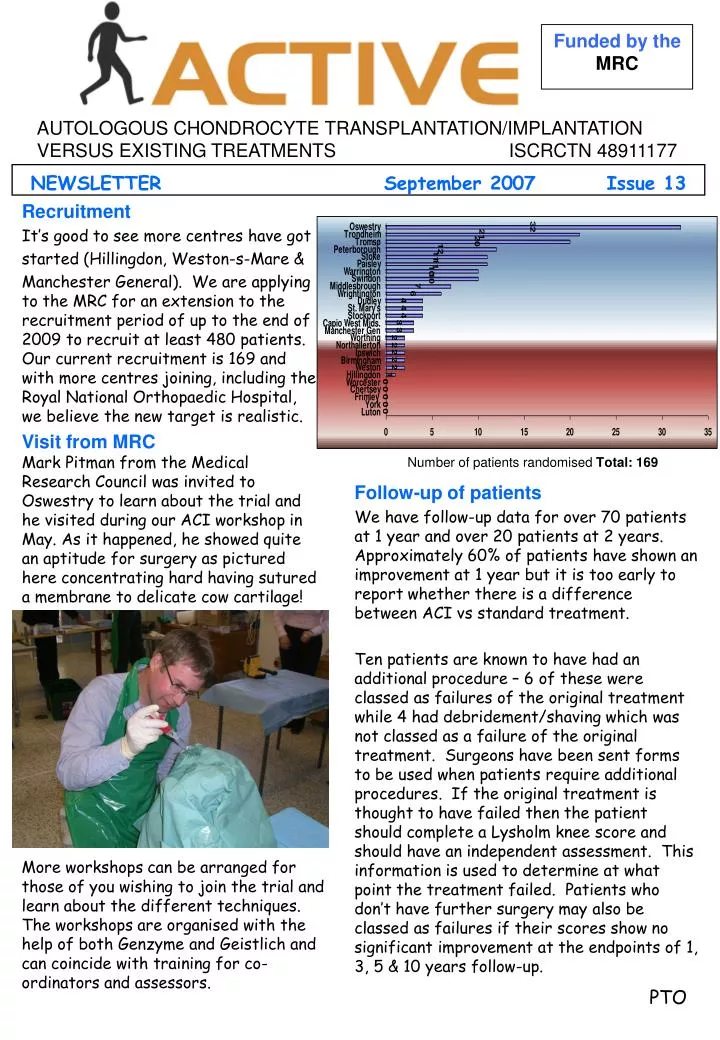
Funded by the MRC AUTOLOGOUS CHONDROCYTE TRANSPLANTATION/IMPLANTATION VERSUS EXISTING TREATMENTS ISCRCTN 48911177 NEWSLETTER September 2007 Issue 13 Recruitment It’s good to see more centres have got started (Hillingdon, Weston-s-Mare & Manchester General). We are applying to the MRC for an extension to the recruitment period of up to the end of 2009 to recruit at least 480 patients. Our current recruitment is 169 and with more centres joining, including the Royal National Orthopaedic Hospital, we believe the new target is realistic. Visit from MRC Mark Pitman from the Medical Research Council was invited to Oswestry to learn about the trial and he visited during our ACI workshop in May. As it happened, he showed quite an aptitude for surgery as pictured here concentrating hard having sutured a membrane to delicate cow cartilage! Number of patients randomised Total: 169 Follow-up of patients We have follow-up data for over 70 patients at 1 year and over 20 patients at 2 years. Approximately 60% of patients have shown an improvement at 1 year but it is too early to report whether there is a difference between ACI vs standard treatment. Ten patients are known to have had an additional procedure – 6 of these were classed as failures of the original treatment while 4 had debridement/shaving which was not classed as a failure of the original treatment. Surgeons have been sent forms to be used when patients require additional procedures. If the original treatment is thought to have failed then the patient should complete a Lysholm knee score and should have an independent assessment. This information is used to determine at what point the treatment failed. Patients who don’t have further surgery may also be classed as failures if their scores show no significant improvement at the endpoints of 1, 3, 5 & 10 years follow-up. More workshops can be arranged for those of you wishing to join the trial and learn about the different techniques. The workshops are organised with the help of both Genzyme and Geistlich and can coincide with training for co-ordinators and assessors. PTO
Non-compliant patients A small minority of patients haven’t been turning up to assessments – if possible can assessors / co-ordinators send the questionnaire pack out by post with a pre-paid envelope so that we at least have this data collected. Data should be collected as close to the scheduled timelines as possible. However, the database will accept data collected early or late within the following timelines: 2/3 month assessment: 8-16 weeks inclusive 6 months assessment: 21-34 weeks inclusive 12 months assessment: 43-64 weeks inclusive Human Tissue Authority regs. Some new regulations came into force in July which affect the procurement, and import/export of human tissue. There has been some difficulty interpreting these regulations and the HTA are meeting with the Department of Health to find a solution, and will meet with us, and Geistlich and Genzyme soon. Meanwhile the HTA has written reassuring us that it will not take any regulatory action against establishments with whom it is in dialogue (the HTA knows which centres are in ACTIVE) and until the matter is resolved activity (i.e. ACI) can continue. Collaboration with the RNOH As mentioned already, surgeons at the RNOH, Stanmore plan to join ACTIVE after finishing recruitment into their ACI/MACI trial later this year. This collaboration will be a very positive step and we look forward to seeing them climb the recruitment league! Tim Briggs has joined the Trial Steering Committee to represent the RNOH and its collaborators. UK-ICRS Meeting A UK-ICRS conference is planned for the spring, to take place at Stanmore, led by Dave Marsh and Tim Briggs – date to be confirmed. ACTIVE Assistant I’m delighted to say that we have a new member of staff – Samantha Griffith-Norris who is helping me in the office with the admin/clerical work and will be able to help answer your queries. Samantha’s telephone number is 01691 404156. Best wishes, Heather Smith ACTIVE Trial Manager Heatherj.smith@rjah.nhs.uk Tel: 01691 404142