Download
1 / 25
250 likes | 442 Views
Case Presentations : Genes and Liver Disease. Victor Ankoma-Sey, MD Director , Liver Transplant Program, Houston Methodist Hospital Director , Liver Associates of Texas, PA. Case # 1. 28YOWF presents with jaundice x 1 week and lethargy PMH: No prior liver disease PSH:Nil

E N D
Case Presentations:Genesand LiverDisease Victor Ankoma-Sey, MD Director, Liver Transplant Program, Houston MethodistHospital Director, Liver Associates of Texas, PA
Case # 1 • 28YOWF presents with jaundice x 1 week and lethargy • PMH: No prior liver disease • PSH:Nil • Meds: Multivitamin • FH: Mother has hypothyroidism • SH: no etoh, no illicit drugs, nonsmoker, single
Case # 1 • P/E: VSS • HEENT:Sclera- icteric, Conj: pallor+ • Chest: Clear • COR : nl • Abdo: nl • Ext: no pedal edema • Neuro: Lethargic , Nonfocal, Asterixis +
What is the Diagnosis? • A. Acetaminophen (Tylenol) Hepatotoxicity • B. Autoimmune Hepatitis • C. Acute Hemolytic Crises with Fulminant Liver Failure in Wilson’s Disease • D. Mushroom poisoning • E. Heatstroke 4
What is the next Step in Mx ? • Start urgent D-Penicillamine treatment • Transfer to Transplant ICU: emergent evaluation for liver transplantation • Start plasmapheresisas an outpatient • Begin Trientine immediately • Initiate IV Acetylcysteine (Mucomyst) 1
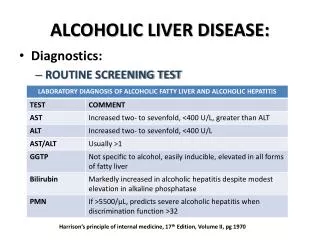
Acute Hemolytic Crises with Fulminant Liver Failure in Wilson’s Disease • Rare presentation of Wilson’s disease • Prompt liver transplantation is crucial to survival • Low alkaline phosphatase and uric acid : are clues • Coomb’s Negative Hemolytic anemia and liver failure: a diagnostic pointer
Case # 2 • A 40 yr Male is brought to ER with hypotension, N/V and diarrhea • PMH: DM, Arthritis • Meds: Metformin, Motrin • FH: Father: CHF and DM • SH: Drinks 4-6 beers/day + 3 martinis x many years, mechanic , married. No illicit drugs or smoking h/o. Lives in Galveston, TX • ROS: Ate raw oysters 2 days prior to admission
Case #2 • P/E BP : 80/40 P:120/min T-102F, RR:22Heent: Sclera- icteric, Conj -pink • Chest: Clear • COR: RRR • Abdo: hepatomegaly+ • Ext: pedal edema- • Skin: bullous skin lesions-purpuric, nonblanching. Tanned skin • Neuro: A & O x3, Nonfocal
What is the most likely diagnosis ? • Acute Alcoholic hepatitis • Acetaminophen Hepatoxicity • Acute Hepatitis A • Vibrio VulnificusInfection in a Hemochromatosis patient with active etoh use • Malingering 1
Case # 3What is his prognosis ? • Excellent • Guarded 1
Vibrio vulnificus • V.vulnificus is concentrated in ocean filter feeders: oysters and clams • Primary Sepsis/septicemia: Acquired from ingestion of raw shellfish • Wound Infection: rapidly progressive , associated with exposure to estuarine waters • Growth of the bacterium is exponential when Fe saturation is > 70%
Vibrio vulnificusPrimary SepsisRisk Factors • Hereditary Hemochromatosis: 12% of patients • Alcoholic cirrhosis: 31-43% of patients • Underlying liver diseases including cirrhosis and chronic hepatitis : 24-31% of patients • Alcohol abuse without documented liver disease: 12-27% of patients • Chronic diseases: DM, RA, thalasemmia major, Chr renal failure and lymphoma: 7-8% of patients
Vibrio vulnificusPrimary Sepsis • 1/3 present in shock or become hypotensive within 12 hrs of admission • Thrombocytopenia and DIC is common • A serious illness:-Among all reported foodborne infections in the US, it is associated with highest case fatality rate (39%)-Case fatality rate > 90% when hypotensive at presentation
Case #3 • 58 y/o Caucasian female referred for > 3 year h/o elevated liver enzymes • C/O fatigue, RUQ abdo pain • Past Medical History • Obesity (BMI:40), DM, hyperlipidemia, HTN, back pain, arthritis, depression • No alcohol history • FH: Mother died from cirrhosis/NAFLD • Meds: • Lipitor, Motrin, Effexor, Norvasc , Metformin
Case #3 • Laboratory • ALT:72 • AST:55 • ALk Phos:115 • Albumin:4.0 • Platelets: 160,000 • INR:1.1 • Fasting insulin:30 • Fasting glucose:100 • HBV, HCV: negative • Fasting iron panel: normal • ANA :80 • ASMA, AMA: negative • TSH: 0.8 • Celiac Panel: - • A1AT level: normal
What are your initial Recommendations • A. Dietary modifications • B. Exercise • C. Cognitive behavior therapy • D. Control DM, Rx Hyperlipidemia • E. All of above 1
Which test will help determine her prognosis in the long term? • CT Scan Liver Protocol • Ultrasound • Liver Biopsy • Serial fasting Insulin Level • Waist circumference 1
NAFLD STEATOSIS STEATOHEPATITIS Alone or non-specific inflammation Hepatic cell injury + Inflammation balloning
NAFLD: At risk for advanced disease • Age > 50 years • Diabetes mellitus-Type II • Metabolic Syndrome • Obesity (BMI > 30) ? • AST or ALT > 2X ULN • Dorsocervical fat pad
NAFLD • Prevalence increasing • Distinction between simple fatty liver and NASH with moderate to advanced fibrosis is important • Non-invasive testing may assist in triaging patients for liver biopsy • Therapeutic options remain focused on improving insulin resistance • Heart healthy, low processed carbohydrate diet to produce deficit of 500-1000 cal/day • Exercise, as adjunct to diet, focusing on aerobic activity for 30 minutes/day
NASH - Pharmacologic options • Most evidence-based data : glitazones • Glitazones improve : certainly steatosis and ALT, inflammation and liver cell injury but not fibrosis • The relationship between hepatic and metabolic improvement need to be better understood • Hepatoprotectants need to be developed • Phase II studies with biochemical end-points are needed • Individualized therapy and integrative approaches with diet and lifestyle modifications need to be optimized
Question Key • The key to my questions are as follows: • A. Case #1: • Ques 1What is Diagnosis? Ans: C • Ques2: Next step.. Ans: B • B. Case #2 • Ques1: Most likely .. Ans:D • Ques2: Prognosis..Ans:B • C. Case #3 • Ques 1..Recs.. Ans: E • Ques 2.. Prognosis: C