Download
1 / 82
820 likes | 835 Views
Explore the structure and functions of the olfactory and optic nerves, along with common lesions and syndromes associated with them. Learn about the intricate pathways and connections in the brain for smell and vision.

E N D
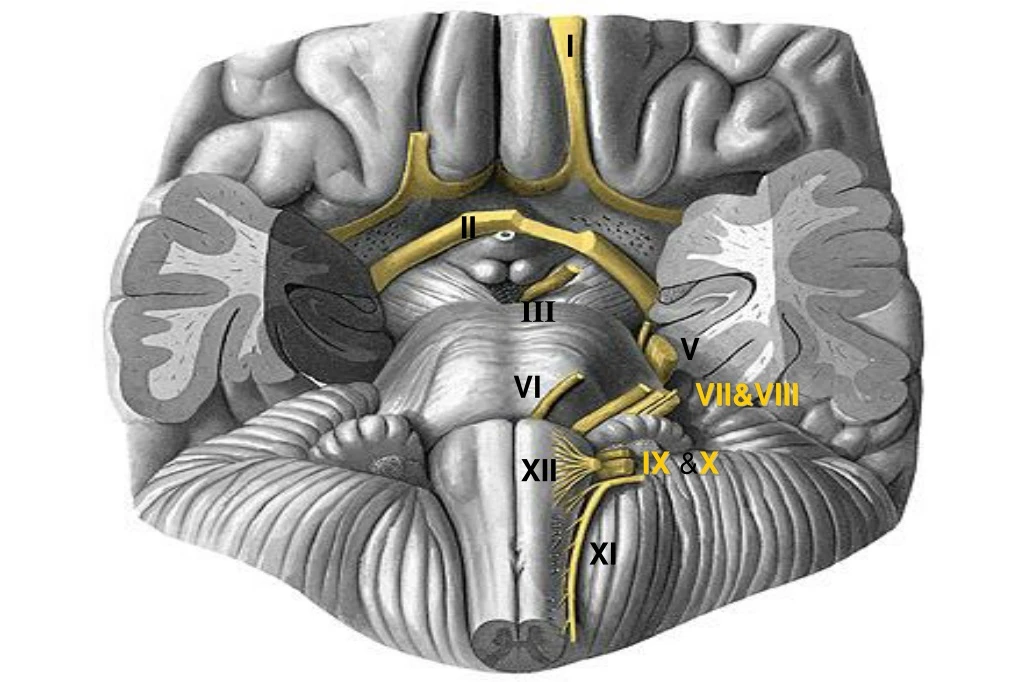
I II III V VI VII&VIII IX &X XII XI
Bulbus olfactorius Cranial NerveI:Olfactory Bipolar cells Foramen: cribiform plate of ethmoid Region Entered: nasal cavity Components: special sensory Target:olfactory epithelium Function: smell 50 million primary sensory receptor cells in 2.5 cm2
Second neurons: First neurons: Unmyelinated 8-20 cilia of 30-200 in length 60 thick layer of mucous (lipid- rich secretion that bathes the surface of the receptors at the epithelium surface) The mucous lipids assist in transporting the odorant molecules as only volatile materials soluble in the mucous, can interact with the olfactory receptors & produce the signals that our brain interprets as odor
Lateral stria anterior olfactory nucleus pyriform cortex nucleus of horizontal limb of diagonal band olfactory tubercle Medial stria transitional entorhinal cortex
Olfactory Tract Connections& Lesion • Lateral stria primary olfactory cortex (periamygdaloid & prepiriform areas) secondary olfactory cortex (entorhinal area (area 28)) • Medial stria cross the anterior commisure to join contralateral olfactory bulb Unilateral anosmia : Compression due to abcess, glioma, meningioma of frontal lob or hypothalamus which may result in ipsilateral optic atropy & contralateral papilledema Foster-Kennedy syndrome
Cranial Nerve II:Opticus Foramen:optic canal of sphenoid Region Entered: orbit Components: special sensory Target, Function: retina-vision
Visual Path 1st neurone: rod & cone cells of the retina 2nd neurone: bipolar neurones of the retina 3rd neurone: multipolar neurones of the retina Axons of the ganglion opticum run via the N. opticus to the chiasma
Visual Path In the chiasma opticum, fibres of the nasal part of the retina cross to the contralateral side, and those of the temporal part continue ipsilaterally Each tractus opticus consists of fibres transporting the information from the contralateral halves of the visual field corpus geniculatum laterale&mediale (some fibres), hypothalamus go directly to the cortex of the brain 4th neurone: corpus geniculatum laterale areas 17&18 around the sulcus calcarinus (area striata)
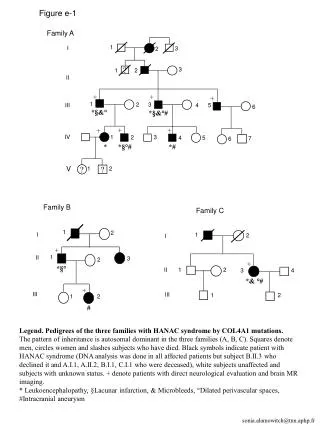
Acute right homonymous hemianopsia in a 59-year-old man due to embolus in the left PCA. (A) MRI shows infarction in the medial left occipital lobe (arrow). (B) Occlusion of the left PCA at its origin (arrow) by an embolus (DSA, left vertebral artery, AP view). (C) The capillary phase (arrow) is absent in the left occipital lobe due to the proximal embolus.
Causes of Papillitis&Retrobulbar Neuritis • Multiple sclerosis • Viral illness; Syphilis • Temporal arteritis & other kinds of inflammation of the arteries (vasculitis) • Poisoning by chemicals: lead, methanol... • Tumors that have spread to the optic n. • Allergic reactions to beestings • Meningitis • Uveitis • Arteriosclerosis
Superior Orbital Fissure Syndrome IV VI III preganglionic parasympathetic to: ciliary ganglion (innervation of sphincter pupillae and ciliary muscle)
Foramen: Superior orbital fissure Region Entered: Orbit Somatomotor Comp.: Target, Function: levator palpebrae sup. superior rectus medial rectus inferior rectus inferior oblique Visceromotor Comp.: preganglionic parasympathetic to: ciliary ganglion Cranial Nerve III: Oculomotor R eye
THIRD CRANIAL NERVE PALSIES • During primary gaze, weakness of • the muscles innervated by, result in: • Ptosis of the lid • Mydriasis • Outwardly turned eye • Pupil is completelyspared: • Myopathy • but all other muscles innervated by the 3rd nerve are affected:diabetic 3rd nerve paresis (ischemic process)
Fixed dilated pupils:3rd nerve compression • - Aneurysm of the post. communicating art • - Trauma • - Intracranial mass lesion • - Increasingly unresponsive patient with • 3rd n. palsy:transtentorial herniation • Neurologic examination with CT or MRI • When CT does not show blood: Lumbar puncture (suspected SAH) • Cerebral angiography: if aneurysmis suspected
+Nuc. Ruber infarction in midbrain Benedict syndrome: contralat. tremor + İpsilat. 3rd n. palsy & fixed pupilla Pupillary Reflex: Afferent: NII Edinger-Westpal nuc. Efferent: NIII parasympath. Argyll Robertson pupil Accomodation Retained Light reflex absent
Horner Syndrome • Ptosis • Myosis • Enophthalmus • Loss of sweating on the affected side of the face From hypothalamus, sympathetic nn. descend ipsilat. through the brainstem & cervical cord & riches the sympathetic chain via the motor root of T1. From there, fibers pass along the outer sheath of the internal carotid artery&its opht.branch &to the pupilla. Fibers to the face travel with the ext. carotid artery Pancoast tm, mass compress. cervical symp. chain
Superior Orbital Fissure Syndrome IV VI III Cranial Nerve IV: Trochlear Foramen: Superior orbital fissure Region Entered: Orbit Components: somatomotor Target, Function:Superior oblique muscle
Cranial Nerve IV: Trochlear Superior oblique muscle palsies • Affect vertical eye position when the eye is turned inward • The patient sees double images: one above & slightly to the side of the other • By tilting the head to the side opposite the palsied m.,the pt may achieve full ocularmotility without double vision • Causes: idiopathic, closed head trauma, aneurysms, tm, MS
Cranial NerveVI: Abducens Foramen: Superior orbital fissure Region Entered: Orbit Components: Somatomotor Target, Function: to lateral rectus (best abductor!)
6th Nerve Palsy • Idiopathic: improvement within 2 mo • Elderly or diabetic pts: small vessel disease • Compression in cavernous sinus: severe • headache& anesthesia in the areaof n.V1 • Increased intracranial pressure: • shift in the brain stretch the 6th n. • Trauma(basilar skull fracture) • Infections &tumors affecting themeninges • Aneurysm,MS • Wernicke's encephalopathy
Saccadic Eye Movements Frontal eye field (FEF & SEF) Medial rectus Lat. rectus Mesensephalon MLF ııı VI ıv Nuc. Abducens Pons P P R F vı VIIIN MLF MLF Retina Optik nerve Corpus geniculatum lat. Area 17. & 19. FEF Mesencephalon Pons (VI. contral. III. & n. nuclei)
Saccadic Eye Movements Frontal eye field (FEF & SEF) Medial rektus Lateral rektus MLF Mesencephalon ııı VI ıv Nuc.VI P P R F Pons vı VIII MLF MLF
Saccadic Eye Movements Frontal eye field (FEF & SEF) Medial rektus Lateral rektus Mesencephalon MLF VI ııı ıv Nuc. Abducens Pons P P R F vı VIII MLF MLF
Vestibulo-ocular Reflexe paths Vertical Gaze Rapid turn of the head to the left • Bilateral control • Center: Dorsal rostral mesencephalon • 3 integral structures: • - riMLF • - Cajal’s interstitial nuc. • - Posterior commisure • Inputs from PPRF & vestibular nuclei • Each riMLF projects ipsilaterally to III & IV n. nuclei Ant. motion of the fluid in the labyrinth Cupula is stimulated Ipsilat. IIIrd & contralat. VIth nerves are stimulated Eyes turn right in order to sustain forward gaze
Cranial Nerve V: TrigeminalV1-Trigeminal ophthalmicMajor branches: Lacrimal, Frontal, Nasociliary & Meningeal Foramen: superior orbital fissure Region Entered:orbit Components:general sensory Target, Function: general sensation from skin and mucosa in region at & above orbit
CorneaReflex • Afferent: N V1 • Efferent: N VII (blink) Ciliary ganglion
V2-Trigeminal maxillary Infraorbital,Zygomatic,Nasopalatine,Palatine Foramen:rotundum Region Entered: pterygopalatinefossa Components: general sensory Target, Function: gen.sensation from skin & mucosa in region from orbit to mouth
V3-Trigeminal mandibularBuccal, Auriculotemporal, Lingual, Inf.alveolar & Meningeal Foramen:ovale with lesser petrosal from CN9 Region Entered: infratemporal fossa Components: brachiomotor Target, Function: muscles of masticat. tensor tympani & veli palatini, mylohyoid ant. belly digastric
Lesion of spinal tractV • IPSILATERAL deficits • in pain & temperature from the face etc. • (the pain information never gets to the • caudal spinal nucleus) • Interruption of the trigeminothalamic tract • deficits in pain &temperature on the • contralateral side of the face • (comprised of axons that have crossed • the midline)
Causes of Sensory Trigeminal Neuropathy • Idiopathic • Systemic inflammatory disease • Sjögren's syndrome • Progressive systemic sclerosis (scleroderma) • Mixed connective tissue disease • Systemic lupus erythematosus • Dermatomyositis • Rheumatoid arthritis • Sarcoidosis • Wegener's granulomatosis • Undifferentiated connective tissue disease • Giant cell arteritis • Idiopathic hypertrophic cranial pachymeningitis • Multiple sclerosis • Tumor • Intracranial or extracranial • Metastatic • Primary: Meningioma, Schwannoma, Epidermoid, Chordoma • Trauma • Aneurysm • Dural external carotid artery cavernous sinus fistula • Sickle ceil disease • Diabetes mellitus • Syringobulbia • Infections • Sinusitis • Herpes simplex • Herpes zoster • Hepatitis A infection • Nonspecific viral infection • Tuberculosis • Whipple's disease • Leprosy • Arachnoiditis • Tricloroethylene • Hydroxystilbamidine • Amyloidosis • Spinal epidural anesthesia
TRİGEMİNAL NEVRALJİ ? Preganglionik sinir kökleri: Subaraknoid alan
Facial NerveTemporal, Zygomatic, Buccal, Mandibular, Cervical&Post. Auricular internal acoustic meatusfacial canalstylomastoid foramen • Brachiomotor:m. of facial expr.: stapedius,stylohyoid, mylohyoid, post.belly digastric • facial canal middle ear chorda tympani petrotympanic fissure • Special sensory: taste, ant. 2/3 tongue: facial canal middle ear chorda tympani petrotympanic fissure • Visceromotor:preganglionic parasympathetic tosubmand. ganglia (innervates submand. &sublingual glands) greater superficial petrosal pterygoid canal pterygopalatine ganglia tolacrimal, nasal & palatine gl.