Download
1 / 29
290 likes | 512 Views
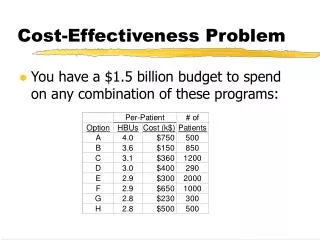
Cost -Effectiveness of AEDs in Office Settings. Jeff Harris Kaileah McKellar Rosanra Yoon John Murphy Rebecca Hancock-Howard Peter Coyte. CPHA– May 29 , 2014. Background. 40,000 SCA per year in Canada. Survival of SCA is 5%. AED are effective at increasing survival.

E N D
Cost-Effectiveness of AEDs in Office Settings Jeff Harris Kaileah McKellar Rosanra Yoon John Murphy Rebecca Hancock-Howard Peter Coyte CPHA– May 29, 2014
Background • 40,000 SCA per year in Canada. • Survival of SCA is 5%. • AED are effective at increasing survival. • The cost-utility in office settings has yet to be examined.
What are AEDs? Automated External Defibrillators
Are AEDs effective? • Survival rate from Sudden Cardiac Arrest (“SCA”) with AED +CPR is approximately doublecompared to CPR alone. • Citizen CPR and rapid defibrillation are the most important factors for survival.2-4
“Marketplace goes on the hunt” “So having a cardiac arrest in a public place and not having an AED is a travesty,” 1
Policy Significance • AEDs are currently not legislatively required in workplaces. • Generally, the public thinks that AEDs are important to have in public and workplace settings. • Federal government departments are exploring policies to make AEDs available in government office buildings.
Research Question Are AEDs cost-effective in Canadian Federal Public Service office settings when compared to employee CPR training?
Approach • Employer perspective • Interventions: • CPR training (current practice). • AED installation and training. • Setting / study population: • Population: 33488 workers. • Setting: Two federal government departments • 657 buildings with >1 worker across Canada
Approach • Cost-utility Analysis • 8-year time period (two AED battery life cycles) • Incremental costs per incremental unit of outcome associated with implementing AEDs together with CPR, compared to CPR training alone • Sensitivity analysis: one-way and probabilistic (Monte Carlo simulation)
Data Collection • Setting/population: Data from two government departments. • Cost data: Environmental scan/web search. • Outcomes data: Literature review.
Model Assumptions • Training costs excluded (AED / CPR offset one another). • Workplaces with only 1 worker excluded. • 1 AED unit per 100 workers per location. • Survival and incidence rates used are reflective of our population. • Threshold ICER of $50,000
Results (ICER) • Calculated ICER = $874,214 Cost/QALY • The cost-effectiveness analysis exceeded the threshold ICER and due to the high cost/QALY would likely exceed the Federal government’s willingness to pay.
Discussion • The results are comparable to other office-based AED studies that calculated ICERs at $511,766 Cost/QALY on a 5 year cycle2. • Other “public-based” studies have calculated ICERs in the range of $30, 000 $10,324,900 Cost/QALY (USD)7.
Strengths and Limitations • Strengths • Actual population data provided more precise estimates • Model uses actual survival data from public locations rather than assumptions based on time to intervention • Limitations • No data available for the physical locations (e.g. number of floors) • Survival and likelihood data from all public settings vs. office only • Limited data on probability that AEDs will be used in office settings • Limited long-term SCA survival data based on the treatment they received
Conclusions • AED are not cost-effective in office settings
References • Dr. Laurie Morrison, a medical researcher who specializes in emergency medicine. Cited by CBC, http://www.cbc.ca/news/health/defibrillators-may-be- hard-to-find-in-emergencies-cbc-investigation-1.2443853 • SharieffW, Kaulback K. Assessing automated external defibrillators in preventing deaths from sudden cardiac arrest: An economic evaluation. International journal of technology assessment in health care 2007;23(03):362-7. • Cram P, Vijan S, Fendrick AM. Cost effectiveness of Automated External Defibrillator Deployment in Selected Public Locations. Journal of general internal medicine 2003;18(9):745-54. • Valenzuela TD, Roe DJ, Nichol G, Clark LL, Spaite DW, Hardman RG. Outcomes of rapid defibrillation by security officers after cardiac arrest in casinos. New England Journal of Medicine 2000;343(17):1206-9. • Vaillancourt C, Stiell IG. Cardiac arrest care and emergency medical services in Canada. The Canadian journal of cardiology 2004;20(11):1081-90. • Nichol G, Huszti E, Birnbaum A, Mahoney B, Weisfeldt M, Travers A, et al. Cost-effectiveness of lay responder defibrillation for out-of-hospital cardiac arrest. Annals of emergency medicine 2009;54(2):226-35. • Nichol G, Valenzuela T, Roe D, Clark L, Huszti E, Wells GA. Cost effectiveness of defibrillation by targeted responders in public settings. Circulation 2003;108(6):697-703. • Weisfeldt ML, Sitlani CM, Ornato JP, Rea T, Aufderheide TP, Davis D, et al. Survival After Application of Automatic External Defibrillators Before Arrival of the Emergency Medical SystemEvaluation in the Resuscitation Outcomes Consortium Population of 21 Million. Journal of the American College of Cardiology 2010;55(16):1713-20.
Review of Provincial and Federal AED Legislation and Guidance
American College of Occupational and Environmental Medicine’s Recommended AED Program Components • Development of a centralized management system for the AED program for managing the AED program and includes establishing roles and responsibilities of various workplace parties. • Medical direction and control of the workplace AED program by a qualified physician or health care provider • Compliance with local, provincial and federal legislation • Development of an AED program for each location where AEDs are to be deployed • Coordination with local emergency medical services • Integration of the AED program with established organizational emergency response plans • Selection technical consideration of AEDs to ensure they meet recognized standards and organizational needs. • Assessment of the proper number and placement of AEDs and supplies so to ensure AEDs and ancillary equipment are located within 5 minutes of a recognized SCA. • Scheduled maintenance and replacement of AEDs and ancillary equipment per manufacturers recommended service schedule. • Establishment of an AED QC/QA program, which should include medical review, record keeping and program evaluation. (29)