Download
1 / 21
220 likes | 344 Views
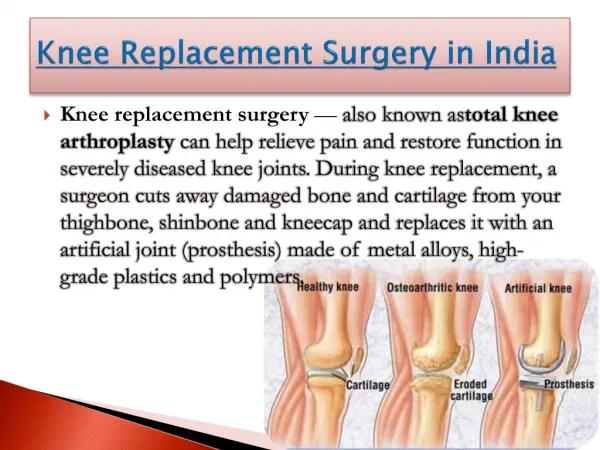
Knee Replacement Surgery Evaluating Rehabilitation Management Strategies Dr Marlene Fransen. The George Institute. Mission Burden of non-communicable diseases and injury Expertise Large scale clinical trials and observational studies

E N D
Knee Replacement Surgery Evaluating Rehabilitation Management Strategies Dr Marlene Fransen
The George Institute Mission • Burden of non-communicable diseases and injury Expertise • Large scale clinical trials and observational studies • Track record in osteoarthritis and orthopaedic surgery clinical research
Outline of Presentation • Epidemiology • Outcomes • Current rehabilitation regimes • Implications for private health insurance • Research proposal
Epidemiology: arthritis • No.1 health problem older Australians • Aging population • Obese population • No cure • Main diagnosis for TKR
Year 2003-2004 Total: 29,899 Private hospital: 20,022 Epidemiology: knee replacements
Private hospitals 1998-1999: 9,957 2003-2004: 20,022 2008-2009: ? Epidemiology: knee replacements
2001 2031 Epidemiology: aging population
Epidemiology • Increasing surgeon confidence in technology • Emerging ‘baby boomer’ cohort • < 65 years at surgery • 2000: 25% • 2003: 30% • 2006: ?
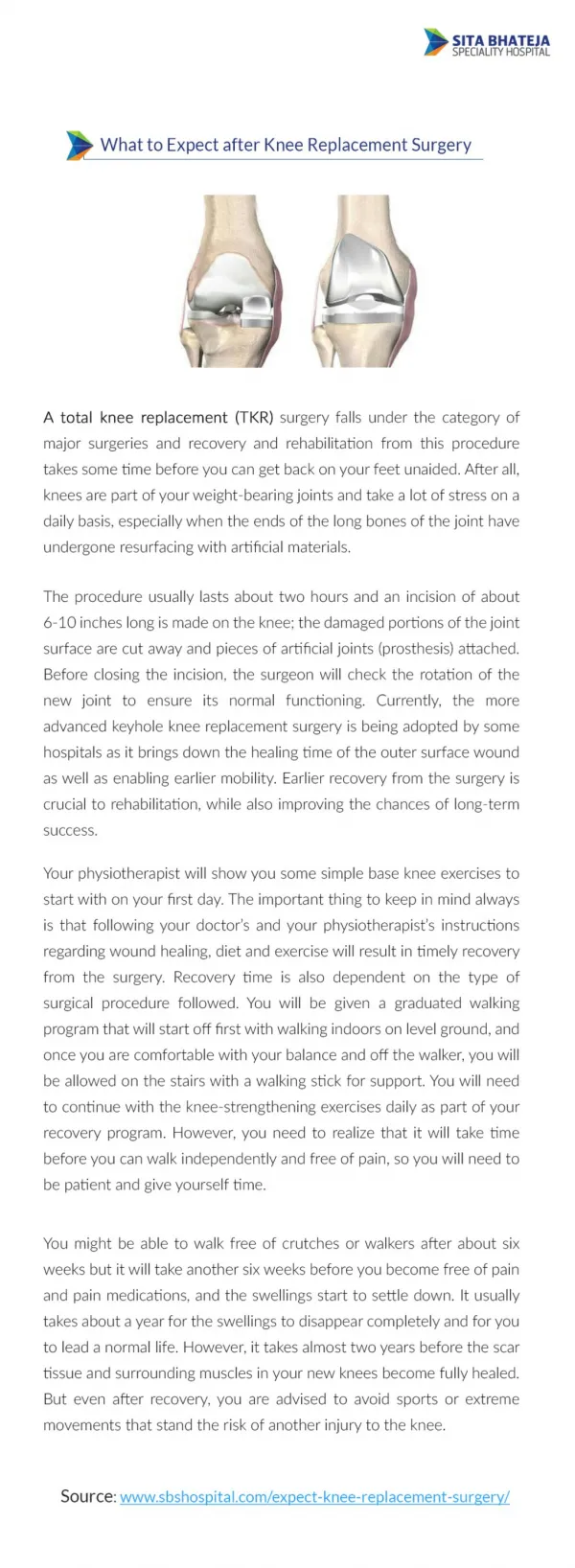
Outcomes Most patients benefit from TKR. Younger patients… • Greater proportion dissatisfied with results • Revision rates markedly higher • Implant survival particularly poor in obese, males
Outcomes Why the difference in outcome? • Continued shortfall in lower limb muscle strength. • Reduced ligamentous constraints. • Higher physical demands. • Longer risk exposure.
Current rehabilitation practice Diversity • Inpatient, outpatient, home visits Consistency • Routine ongoing referral • Mostly 1:1 provision • Mostly completed within 8 weeks of surgery
Effectiveness of rehabilitation? • Few randomised clinical trials (5) • Small studies (n<100) • Short term outcomes (3-6 months) • Inappropriate outcomes (ROM) • Most conclude no evidence of benefit
Supporting costly programs with no evidence of: benefit need for 1:1 treatments usefulness of early treatment Implications for private health insurance
Determine effectiveness and cost-effectiveness of ‘shifting’ outpatient rehabilitation following TKR. Research Aim
Orthopaedic surgeons Physiotherapists Rheumatologists Clinical trials Epidemiologists Health economist Biostatisticians Randomisation centre Data management Project management Patient advocate 12 large hospitals Collaborators
Prevention of chronic ectopic bone-related pain and disability after total hip replacement with peri-operative NSAIDs RCT conducted amongst 902 patients in 20 orthopaedic centres in Australia and NZ . Funded: NH&MRC and MBF Current Research
Risk of EBF Clinical outcomes 6-12 months after surgery Bleeding events during admission period and prolonged hospitalisation Recommendations Current Research
Current Research Glucosamine study RCT 900 patients Early OA knee 1500mg GS/placebo Two years Main outcomes • Pain, function • Joint space
Conclusion • There is no convincing evidence for the effectiveness of rehabilitation after TKR. • The costs for post-acute care are likely to be substantial and will increase rapidly. • Research is urgently required to develop cost-effective rehabilitation regimes. www.thegeorgeinstitute.org