Download
1 / 25
330 likes | 1.08k Views
Energy Metabolism of the Brain. Cerebrospinal Fluid. František Duška. Overview. Brain metabolism energy metabolism ammonia handling Blood-brain barrier Cerebrospinal fluid. Brain metabolism. (except neurotransmiter metabolism – next lecture) Energy metabolism of the brain

E N D
Energy Metabolism of the Brain. Cerebrospinal Fluid František Duška
Overview • Brain metabolism • energy metabolism • ammonia handling • Blood-brain barrier • Cerebrospinal fluid
Brain metabolism (except neurotransmiter metabolism – next lecture) Energy metabolism of the brain Ammonia handling
Energy metabolism of the brain • 2% of body weight, 20% of energy expenditure • GLUCOSE is the main fuel • daily consumption 120g • adopted starvation (3 weeks): oxidation of ketones in the brain covers up to 50% of energy
What´s the first thing that happens when you think? • Excitatory firing Glu uptake by glia Na+ influx ATP consumption by Na-K-ATPase activation of glycolysis lactate transported to neurons • Local increase in lactate increases blood flow • Excitotoxity = excesive Glu release • epilepsy, traumatic brain injury • Na+ and Ca2+ IC accumulation swelling
Functional imaging of ther brain • PET = positron emission tomography • 18F-2-deoxy-2-fluoroglucose • taken up by glia, phosphorylated but not further metabolized • active areas of the brain accumulate tracer
Oxygen uptake • Brain: 20% of whole-body O2 consumption • The most vulnerable to hypoxia • 5 min of VF/arrest may lead to irreversible brain damage • temperature dependent • Clinical use: • jugular venous oxymetry • tissue pO2
Ammonia handling in the brain • NH3 is a waste product of deamination reactions (GlnGlu, Glu2-OG etc.) • Metabolism: • Glutamin synthetase: NH3 + Glu Gln • Gln is metabolized in the liver/kidneys • Ammonia toxicity: NH3 + 2OG + NADH Glu + NAD+ • Krebs cycle impairment: 2-OG depletion • Glu excess, excitotoxicity
Ammonia handling • Clinical consequences: liver disease impairs brain function • principle: insufficient urea synthesis NH3 accumulationneurotoxicity • Hepatic encephalopathy: gr.I-IV • Fulminant liver failure (i.e. paracetamol poisoning) threatens live also by ICP
Blood brain barrier • History: • 19th century, Ehrlich: aniline dye i.v. stains all organs except brain • 1960: morphology by electron microscope • Function: • BBB selectivity protects the brain
Blood brain barrier • Morphology: endothelium, BM, astrocyte
Blood brain barrier selectivity • Free permeability (passive diffusion): • small molecules: H2O, O2, CO2, NH3, ethanol • lipid soluble molecules: steroid hormones • Carrier mediated transport: • glucose: GLUT-1 (insulin independent) • amino acids • Pinocytosis
Areas outside BBB • Enables brain to sense and regulate blood composition • Include: • Subfornical organ: osmoreceptors, regulate ADH • OVLT: dtto, thirst • Area postrema: chemoreceptors, vomining center
BBB – clinical significance • CNS infection: • BBB protects against bacteria entry, but also antibodies and antibiotics • Kernikterus: • hyperbilirubinemia damages the brain in neonates but not in adults • Parkinsons disease: • =lack of dopamin in basal ganglia • cannot be treated with dopamin (does not cross BBB), but its precursor L-DOPA is useful
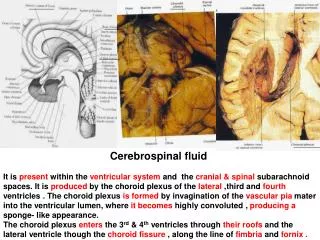
Cerebrospinal fluid Function and circulation Collection and laboratory assessment
Cerebrospinal fluid • Volume = 150 ml, daily production = 500ml • Function: • mechanical protection • distribution of neuroendocrine factors • „volume buffer“: helps to regulate ICP when tissue or intracranial blood volume rises (Monroe-Kelly doctrine: V-CSF+V-blood+V-brain tissue = const.)
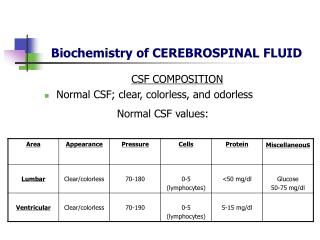
CSF normal composition CSF does not contain cells (normal: up to 5 WBC/l)
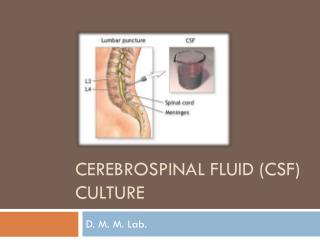
CSF collection for dg. purposes • Lumbar puncture (rarely suboccipital puncture) • 4 samples (2 ml): • biochemistry: ions, Glc, lac, proteins incl. ELFO • cytology: No of RBC and WBC/l event. incl. differential count • bacteriology: standard culture and/or PCR • 1 backup sample stored at 4°C
CSF in diagnostics • CNS infection • bacterial meningitis: voscous and opalescent CSF, WBC, Glucose, Lac • viral meningitis: few cells, protein • Degenerative diseases • oligoclonal bands in multiple sclerosis • others • Hematologic malignancy • leucemic cells infiltrate CNS