Download
1 / 80
800 likes | 959 Views
Dr Bernard Stacey Southampton General Hospital. OESOPHAGEAL CANCER 3rd year SSU. INTRODUCTION. Incidence of adenocarcinoma of the oesophagus is fastest rising cancer in Western world Majority present late when only palliation possible

E N D
Dr Bernard Stacey Southampton General Hospital OESOPHAGEAL CANCER3rd year SSU
INTRODUCTION • Incidence of adenocarcinoma of the oesophagus is fastest rising cancer in Western world • Majority present late when only palliation possible • Resection implies a major procedure and many have concurrent disease
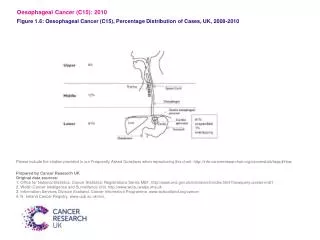
Incidence of Oesophageal Cancers Blot WJ et al. JAMA 1991;265:1287-9
The lower oesophagus: pressure control mechanisms • Lower oesophageal sphincter • Crural diaphragm • Sling fibres of the stomach
Oesophageal wall histology Circular Longitudinal distance in lower oesophagus
Oesophagitis as a cause of oesophageal shortening • Experimental oesophagitis • Distal peristaltic contractions disappear • LOS pressure by 60% • Oesophagus 1-2cm shorter • Oesophageal compliance by 30% • Largely recovered by 4 weeks Zhang X et al. Am J Physiol Gastrointest Liver Physiol; 2005
The longitudinal muscle of the oesophagus • Attached to hypopharynx and diaphragm • At lower end it blends with phreno-oesophageal ligament • More muscle bulk than circular muscle • Can shorten oesophagus by 5-6cm
Anatomy of the Esophagogastric Junction Mittal, R. K. et al. N Engl J Med 1997;336:924-932
The phreno-oesophageal ligament: Origin - fascia transversalis Insertion: oesophageal wall Rich in collagen and elastic fibres
Obesity: challenges OGJ integrity • BMI and waist circumference correlates to in: • intra-gastric pressure and • G-O pressure gradient • Also separation of LOS and crural diaphragm = perfect scenario for reflux
Does weight loss help reflux? • Remarkably little data! • Yes: Derby 1999 • 23 pts BMI >23, GORD 6/12 • - 80% lost wt and symptoms improved • r = 0.548, p<0.001 • No: Stockholm 1996 • 20 pts; pH study confirmed reflux • - no significant improvement despite mean of 10kg wt loss • Maybe: Amsterdam 2002 • 42 pts BMI 43 • - wt loss, no gastric distension improved • - with gastric distension continued reflux
One extra oesophageal adenocarcinoma for every 5000 men over 60 treated
Symptomatic GORD as a risk factor for oesophageal adenocarcinoma • Lagergren J. NEJM 1999; 340: 825-31 Oes Cardia Recurrent symptoms 7.7 2.0 ‘Long-standing’ reflux 43.5 4.4
The oesophagitis-metaplasia-dysplasia-adenocarcinoma sequence 95% don’t present 10% 3.5% 1.2% 100% of adults >30yrs Normal oesophagus Mild Oesophagitis Severe Oesophagitis Barrett’s Metaplasia months months days - weeks years Roleof chemoprevention ? 0.25% 0.08% 0.06% High Grade Dysplasia Adenocarcinoma Low Grade Dysplasia 2 - 5 years 0 - 3 years
‘Natural history’ of HGD • 43% had Ca in resection specimen • 24% progressed to Ca during 2-46 months follow up • Ca incidence at 3 yrs • 56% if diffuse • 14% if focal HGD • Veterans’ study – 7.3 yrs F/U: 4 / 79 Ca in 1st year 12 / 75 Ca of whom 11 cured • But: single pathologist
Reflux, Barrett’s and cancer • ~10% of population have reflux • 10-15% of these have Barrett’s change (short > long segment) • These get adenocarcinoma at 0.5%/year • 40% of adenocarcinomas have no history of GORD • <5% of adenocarcinomas are known to have Barrett’s on presenting with symptoms of their cancer
Symptomatic GORD as a risk factor for oesophageal adenocarcinoma • Lagergren J. NEJM 1999; 340: 825-31 Oes Cardia Recurrent symptoms 7.7 2.0 ‘Long-standing’ reflux 43.5 4.4
Dysphagia • Weight loss • Nausea and vomiting • Pain uncommon (unless metastases)
STAGING Stage TNM 1st seen 5yr surv 1 T1 N0 M0 10% 90% 2a T2/3 N0 M0 25% 50% 2b T1/2 N1 M0 3 T3 N1 M0 45% 15% Any T4 4 Any M1 20% 0%