Download
1 / 60
600 likes | 792 Views
Moving From Volume to Value. Benjamin Hohmuth, MD, MPH, SFHM Director , Hospital Medicine Geisinger Medical Center Danville, PA. Learning Objectives - 1. Understand the concepts of volume and value Be aware of key reports/initiatives that have provided support for health reform.

E N D
Moving From Volume to Value Benjamin Hohmuth, MD, MPH, SFHM Director, Hospital Medicine Geisinger Medical Center Danville, PA
Learning Objectives - 1 • Understand the concepts of volume and value • Be aware of key reports/initiatives that have provided support for health reform. • Understand how payment paradigms areevolving and identify some of the associated system and culture changes taking place.
Learning Objectives - 2 • Understand the value proposition for patient blood management
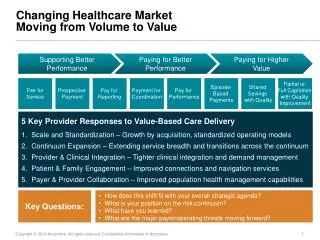
Volume vs Value • Volume Based Reimbursement • Rewards care that involves many transactions • Value Based Reimbursement • Rewards care that is high quality and low cost • V=Q/U
The Call for Change • Institute of Medicine Reports • NEJM - Quality of Health Care • Institute for Health Care Improvement • Dartmouth Atlas of Healthcare • Soaring health care costs
To Err is Human- Building A Safer Health System • Institute of Medicine (IOM) in 1999 • 44,000 - 98,000 people die each year as result of medical errors • Not a “bad apple” problem, we’re only human • It’s about systems
Crossing the Quality Chasm: A New Health System for the 21st Century • IOM 2001 • Our system is broken and needs redesign • 6 aims for improvement • Safe • Effective • Patient Centered • Timely • Efficient • Equitable
“We have no comprehensive view of the level of quality of care given to the average person in the United States. This information gap contributes to a persistent belief that quality is not a serious national problem” NEJM 2003 348;26:2635-2645
<45% of patients were found to have received recommended care NEJM 2003 348;26:2635-2645
Institute for Healthcare Improvement • 100,000 Lives Campaign • Don Berwick • The Triple Aim • Improve Health • Improve Care • Decrease Costs
Dartmouth Atlas of Health Care • Jack Wennberg • Unwarranted variation • Dartmouth Atlas • Medicare spend per beneficiary • Quality of care delivered
Dartmouth Atlas of Health Care Science. 1973 Dec 14;182(4117):1102-8
Medicare Spending per Beneficiary Dartmouth Atlas of Healthcare ’09
Rates of Effective Care Delivery Dartmouth Atlas of Healthcare ’09
Health Care Costs • 2011 • 2.7 trillion dollars • 17.9% of GDP • $8,660 per capita • Average family premium >$15,000 • Costs vs Revenue • Who pays? SOURCE: Centers for Medicare & Medicaid Services, Office of the Actuary.
Health Care Costs – Who Pays? 2013 Milliman Medical Index
Source: Organisation for Economic Co-operation and Development (2010), "OECD Health Data", OECD Health Statistics (database).doi: 10.1787/data-00350-en(Accessed on 14 February 2011). Notes: Data from Australia and Japan are 2007 data. Figures for Belgium, Canada, Netherlands, Norway and Switzerland, are OECD estimates. Numbers are PPP adjusted.
Overall Ranking US vsOther High Income Note: * Estimate. Expenditures shown in $US PPP (purchasing power parity). Source: K. Davis, C. Schoen, and K. Stremikis, How the Performance of the U.S. Health Care System Compares Internationally 2010 Update, (New York: The Commonwealth Fund, June 2010).
OECD 2011 OECD 2011
The Problem • We are spending lots of $$$ • There is wide regional variation • We are causing harm • Not providing appropriate care • Providing inappropriate care • More $$$ ≠ better health outcomes • We have no system • Insufficient return on investment
Culture and System Changes The Past The Future Payment for performance (active purchaser of health) Measurement and public reporting Standardization of care Physician is a team member Delivery is integrated Interdependence of physicians and hospitals • Transaction based payment (passive payer of services) • No measurement or public reporting • Variation in care • Physician is autonomous • Delivery is fragmented • The hospital as the physicians workshop
Optional P4P • Patient Centered Medical Home • ACO’s via shared savings provision • ACO’s via CMMI • Bundled Payments
Required P4P • HOSPITAL PROGRAMS • Hospital Value Based Purchasing • Hospital Readmission Reduction Program • Hospital Acquired Conditions Penalty • Meaningful Use Incentives/Penalties
Hospital Value Based Purchasing • Impacts Payments FY 2013 (Oct 2012) • Funded by DRG cuts effective Oct 2012:
Hospital Readmission Reduction Program • Impacts Payments FY 2013 (Oct 2012) • Conditions: CHF, MI, PNA
Hospital Acquired Conditions • Starts FY 2015 • Top quartile hospitals penalized • 1% DRG reduction
Meaningful Use • 2011 first year of incentive • 2015 penalties begin • 2017 penalties fully phased in
Cumulative Financial Impact • Oct 2013 – 3.25% at risk • Oct 2014 – 5.5% at risk + MU penalty • Medicare Part A
Required P4P • PHYSICIAN PROGRAMS • Physician Quality Reporting System • E-prescribing • Meaningful Use Incentives/Penalties • Physician Value Based Purchasing
Required Physician P4P PHYSICIAN VALUE BASED PURCHASING • 2015: apply modifier to specific physicians. • 2017: apply modifier to all physicians
Culture and System Changes The Past The Future Payment for performance (active purchaser of health) Measurement and public reporting Standardization of care Physician is a team member Delivery is integrated Interdependence of physicians and hospitals • Transaction based payment (passive payer of services) • No measurement or public reporting • Variation in care • Physician is autonomous • Delivery is fragmented • The hospital as the physicians workshop
Culture and System Changes The Past The Future Payment for performance (active purchaser of health) Measurement and public reporting Standardization of care Physician is a team member Delivery is integrated Interdependence of physicians and hospitals • Transaction based payment (passive payer of services) • No measurement or public reporting • Variation in care • Physician is autonomous • Delivery is fragmented • The hospital as the physicians workshop
Variation to Standardization • Standardization of care for populations • Physicians must justify variation for individuals • Why no betablocker after surgery? • Why was a urinary catheter left in? • BUT “I forgot” or “I don’t believe in that” will not justify variation
Culture and System Changes The Past The Future Payment for performance (active purchaser of health) Measurement and public reporting Standardization of care Physician is a team member Delivery is integrated Interdependence of physicians and hospitals • Transaction based payment (passive payer of services) • No measurement or public reporting • Variation in care • Physician is autonomous • Delivery is fragmented • The hospital as the physicians workshop
Cowboy to Pitcrew • Physicians will be an important member of a multidisciplinary health care team • Team hierarchies will be flatter • Surgical time outs • Central line associated blood stream infections • The importance of the company we keep
Culture and System Changes The Past The Future Payment for performance (active purchaser of health) Measurement and public reporting Standardization of care Physician is a team member Delivery is integrated Interdependence of physicians and hospitals • Transaction based payment (passive payer of services) • No measurement or public reporting • Variation in care • Physician is autonomous • Delivery is fragmented • The hospital as the physicians workshop
Fragmentation to Integration • Managing care require coordination • Horizontal integration • Hospitals merging, acquiring docs • Vertical integration • Providers taking risk, insurers buying providers • Successful organizations will control the continuum of care
Culture and System Changes The Past The Future Payment for performance (active purchaser of health) Measurement and public reporting Standardization of care Physician is a team member Delivery is integrated Interdependence of physicians and hospitals • Transaction based payment (passive payer of services) • No measurement or public reporting • Variation in care • Physician is autonomous • Delivery is fragmented • The hospital as the physicians workshop
Independence to Interdependence • Hospitals Looking for Help from Physicians • Clinical documentation • Maximize DRG • POA vs HAC • Variation from care standards • Surviving RACs and MACs - Medical necessity • LOS, cost per case, readmissions • Managing the continuum of care
Independence to Interdependence • Physicians Looking for Help from Hospitals • Declining revenue • Limited leverage • Accountability for outcomes that depend on multiple actors and complex systems • Risk Management • Financial uncertainty
Independence to Interdependence • A new business model • Rapidly increasingphysicianemployment • Pro vs facility fees • Managing utilization and quality