Download
1 / 14
140 likes | 151 Views
This chapter explores the clinical aspects of specific organ transplants, including cornea, kidney, liver, heart, lung, pancreas, intestine, and heart/lung. It provides an overview of the different types of tissue transplants, mechanisms of immune rejection, and the primary anti-rejection therapies used in transplantation. The chapter also discusses the importance of MHC matching and the role of cross-matching in avoiding hyperacute rejection.

E N D
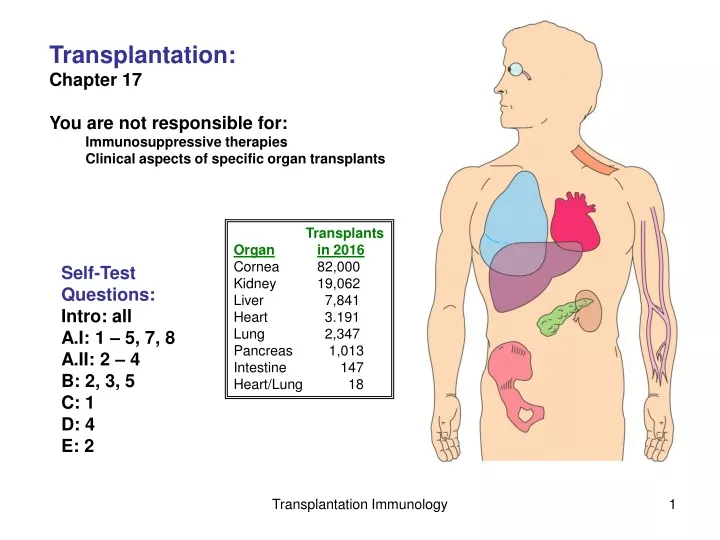
Transplantation: Chapter 17 You are not responsible for: Immunosuppressive therapies Clinical aspects of specific organ transplants Transplants Organin 2016 Cornea 82,000 Kidney 19,062 Liver 7,841 Heart 3.191 Lung 2,347 Pancreas 1,013 Intestine 147 Heart/Lung 18 Self-Test Questions: Intro: all A.I: 1 – 5, 7, 8 A.II: 2 – 4 B: 2, 3, 5 C: 1 D: 4 E: 2 Transplantation Immunology
What are different types of tissue transplants? Sources -- Living donor; & self -- Cadaver -- Animal Autologous graft -- e.g., skin, artery transplants -- not rejected Isograft -- e.g., any organ -- not rejected Allograft -- kidney, liver, heart transplants -- rejected; unless Im privileged Xenograft -- rejected, unless non-antigenic -- e.g., heart valves Transplantation Immunology
There are three types of Transplant rejection Host-vs-Graft Hyperacute rejection -- rapid: minutes to hours -- preexisting antibodies -- massive antigenic differences -- blood types; MHC -- xenografts Acute rejection -- killer T-cells -- days/weeks/months -- MHC rejected as foreign Chronic rejection -- years -- despite immunosuppressive therapy -- Minor Genetic Differences Different people will have different types of MHC Graft-vs-Host can also occur Transplantation Immunology
What are the mechanisms of Immune rejection Direct vs Indirect allo-recognition Effector cells Rejection mechanisms Transplantation Immunology
What causes ‘Direct’ allo-recognition? Primary mechanism of rejection (10x greater than indirect) Recipient T-cells are activated by: Graft-MHC + Graft peptides Why would T-cells bind to peptides in non-self MHC? Graft-MHC + peptide can resemble … Self-MHC + foreign peptide May contribute mostly toward acute rejection MHC + peptide Transplantation Immunology
What causes ‘Indirect’ allo-recognition? Recipient T-cells are activated by recipient MHC + graft (MHC) peptides Analogous to normal T-cell response to pathogens (or vaccines) -- Recipient macrophages enter transplant -- Phagocytose cellular debris -- Present to & activate recipient Thand T-killer cells -- T-killer cells attack transplant May contribute mostly toward chronic rejection -- graft DCs soon removed from body Transplantation Immunology
There presently is no way to avoid chronic rejection? “Minor histocompatibility proteins” -- allogenic differences Slow, progressive onset of immune response to transplant Tissue rejection has memory! 5 Year survival rate (2009) Kidney: 69% Heart: 75% Liver: 75% Lung: 54% Transplantation Immunology
When does Graft vs Host Disease (GvHD) occur? -- bone marrow -- some solid organ Immune cells of graft react against recipient tissues -- Allo-reactive antibodies -- Cell-mediated attack Occurs in 75%+ of bone marrow transplants But has beneficial effect against leukemic and cancerous cells Transplantation Immunology
Minimizing MHC differences between donor and recipient reduce hyperacute & acute rejection -- a sibling may be closest match Tissue matching – methodology that determines the types of MHC present on donor and recipient cells Some MHCs more important than others -- MHC-A, B & DR Reduces acute rejection Transplantation Immunology
2. HLA (tissue) matching a) Serological -- use HLA specific mABs b) DNA analysis -- look for HLA-allele specific sequences Not all HLA tested for… Why? HLA typing at NY Blood Center Serology HLA Class I (A,B,C) HLA Class I HLA-B27 DNA analysis PCR- broad allele class resolutionHLA Class I (A,B,C) DNA sequencing allele level resolution, HLA Class I (A,B,C) by HLA-Class II (DRB1)HLA-Class II (DQB1) http://www.nybloodcenter.org/HLA-Typing.do?sid0=92&page_id=185 Transplantation Immunology
Not all HLA genes are equally important Why? In Kidney -- Little MHC-II expressed 6 HLA antigens examined: -- HLA-A, HLA-B, and HLA-DR e.g., HLA-A1 & A2, B7 & B8, DR2 & DR3 Liver-- little MHC-I or -II expressed -- usually only ABO matched What about… Cornea:No matching …Why? Heart:No matching …Why? Increased HLA matching yields only minor improvements in kidney survival Transplantation Immunology
Cross matching helps to avoid hyperacute rejection Determines if recipient has antibodies against transplant Can detect presence of all sorts of anti- donor antibodies Transplantation Immunology
What are the primary anti-rejection therapies? 1. Corticosteroids,e.g., prednisone 2. Anti-proliferatives, e.g., azothrioprine 3. T-cell signaling/activation disruptors a) chemotherapeutic agents -- IL-2 inhibitors; e.g., cyclosporine-A, rapamycin b) humanized Mabs -- anti-CD3 -- anti-IL2r (e.g., basiliximab) -- anti-CD20, a B-cell AG) (e.g., rituximab) c) fusion molecules -- B7 antagonist (blocks B7/CD28 interaction) -- e.g., Belatacept; CTL-4 + IgG FC Cyclosprine-A Transplantation Immunology
Organ perfusion prior to transplant can minimize direct acute rejection -- why? -- also improves organ performance What are some experimental anti-rejection therapies? 1. Bone marrow HSC transplants -- transplant HSC from done to recipient 2. Thymic manipulation -- inject donor AG into recipient thymus 3. Treg cell induction -- in vitro or in vivo 4. and others… Transplantation Immunology