Download
1 / 46
2.41k likes | 6.42k Views
Case conceptualization. A case conceptualization model for supervision: Tools for understanding our clients and contexts. David X. Swenson PhD LP MSSA, 2014. Agenda. Rationale for case conceptualization in supervision Problems & cautions in Dx Model for case conceptualization

E N D
Case conceptualization A case conceptualization model for supervision: Tools for understanding our clients and contexts David X. Swenson PhD LP MSSA, 2014
Agenda • Rationale for case conceptualization in supervision • Problems & cautions in Dx • Model for case conceptualization • Variety of tools for identifying & organizing case information • Components of a good case conceptualization • Implementing the case conceptualization
How the client presented the problem & need How the therapist understood it How the case manager summarized it How collateral sources viewed it How the billing agency classified it How treatment was documented How treatment was applied How insurance was billed How it was supported What the client really needed
Pressure to find the “Quick Fix” • Need Dx for insurance coverage & billing • Dx for program and service eligibility • Insistence by client on problem definition • Competition with other agencies for clients • Limited funding for number of sessions • Limited time for session length • Limited access or insufficient time for assessment • Inexperience in diagnostics & case conceptualization • Specialization– “if all you have is a hammer, everything looks like a nail”
ADHD! The Risk of “Drive-By” diagnoses Bipolar! FASD! • Insurance requires diagnosis • Limited background information • Limited exposure to client • Potentially biased information • Only DSM criteria met (no differential Dx) PDD! ODD! • Many NOS & R/O • Multiple diagnoses • Inconsistent diagnoses • Changing diagnoses • No explanation of reasoning • No differential diagnosis • Diversion from more effective treatments • Ineffective interventions • Frustrated staff • Discouraged clients • Medication side effects & interactions • Expense without results
Take time to understand the system that supports the expression of the problem Furthermore…”when you have 20 days to find an answer to a problem, spend the first 19 days understanding the question.”
The Role of Supervision • Enhance clinical skills, knowledge, & attitudes for more effective delivery of services • Understand how to integrate diverse information into a case conceptualization of the client and situation (“working model”) • Developing awareness & coherence of therapy approach & style • Ensure consideration of ethical issues and practice within ethical guidelines • Promote development of critical thinking and clinical judgment • Role model professional conduct and skills in working with clients • Preparation for examinations & documentation for licensure
Why case conceptualization? • Minimize bias, rush to diagnose, & misplaced effort • To integrate multiple perspectives on case • Logically and sequentially “build” the case • Differential Dx & sort out co-morbid disorders • Develop a working model of the client to guide intervention & identify leverage points • Ensure essential information is available and identify missing/needed information
Why case conceptualization cont’d • Provide structure for generating hypotheses • Ensure that all staff are unified in treatment focus • To identify treatment amenability, focus, priorities, and approach treatment in a systematic way • Help therapist anticipate problems that can arise • Communicate the case and treatment clearly to others • Shared with the client can strengthen therapeutic alliance, motivation & compliance
The Wandering Case • Attending late, unprepared • Uncertain what the goals are • Prolonged socializing & off-topic discussion • Interruptions & off on tangents • Repetition of discussion areas • Side discussions • Brainstorming with no decisions • Leaving frustrated and without answers to questions
A procedure for case supervision & consultation • Group supervision: Go-around– who needs what? What is urgent? • What do you need from this discussion? What are your questions? • Discussion Format • Identifying information (age, gender, ethnicity, presenting problem, referral, other agencies) • Capacity (IQ, neurological status, developmental status, functional level) • Background to current question (previous behavior & Dx, family MI history, onset & course of Sx, previous Tx, testing, differential Dx • Tools • Genogram, ecomap, time line, symptom clustering, systems map, family system map, force-field analysis, etc. • Tx Plan • Base rates of key behaviors & goals • Strategy: previous Tx: what worked, what didn’t & why? • Strategy: amenability, leverage, timing, intervener(s) • Follow-up next session for continuity
What symptoms have you observed or hear others complain about that suggests ADHD?
PTSD • Anxiety • Depression • Insufficient sleep • Cognitive impairment • Medication side effects • Learning disability • Autistic spectrum • Substance abuse • Toxic conditions • Health problem • Brain injury • FAS/FAE When is apparent behavior not due to an apparent cause? Inattention, hyperactivity, Impulsivity… ADHD?
Normal kids who have insufficient sleep may present sleep deficit behaviors, easily mistaken for a variety of conditions
Apparent behavior may not be the source to be treated • Insufficient sleep due to • Domestic disturbance • Parents return home late drunk • Hx of sexual abuse by family friend • Inconsistent discipline due to: • Never having learned consistent parenting • One parent compensating for the other parent’s extremes • Parental inattention or forgetfulness Irritable & Defiant Behavior at School • Fatigue • Frustration • Fear • Resentment • Family conflict • Domestic abuse • Threats of divorce
Presence of an event does not necessarily make a disorder • Event • Premature birth • Infant surgeries • Collicky • Difficult to console • Neglected cuddling & food • Mother often ill • Mother jailed • Exposed to domestic abuse • Passed to extended family • Modifiers • Extended family consistent in availability, nurturance • High consistency & structure in home • Socialization modeling Reactive Attachment Disorder ? • Disinhibited RAD: Indiscriminate in approaching others? • Inhibited RAD: Indifferent to others?
We should not assume that all trauma exposure results in PTSD 10-30% 5-10% 15-35% 50-90%! 35-55% Bonanno, G. A. (2004). Loss, trauma, and human resilience: Have we underestimated the human capacity to thrive after extremely aversive events? American Psychologist ,59(1), 20-28. Choe, I. (2005). The debate over psychological debriefing for PTSD. The New School Psychology Bulletin, 3(2), 71-82.
Sources of Information • Multiple sources: client self, parents, extended family, teachers, legal, medical, etc. • Multiple methods: records, tests, observation • Multiple settings: home, school, community • Multiple events: several specific incidents; possible patterns • Over extended time: birth, early through late childhood, adolescence • Level of authority (reliability/validity) of the sources; how accurate? The more information, the more complex but more accurate and thorough; Identify the patterns that persist
Some techniques for organizing the case conceptualization information • Genogram • Timelines • Time & factor information grid • Symptom clustering • FACES Circumplex • Behavior cycles & System mapping • Force-field analysis • Case conceptualization
It’s all perspective… What are the factors that contributed to the emergence of the behavior? How is it currently presented? What are the barriers to change? Where is leverage & amenability? How has it developed over time? How has it responded to intervention? Onset Nature & Course Current Presentation
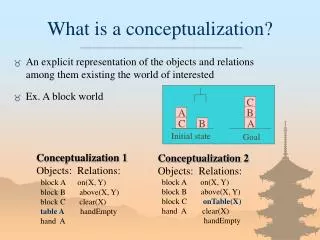
Genogram: Transgenerational family structure & conditions • Family “players” • Hierarchy & lineage • Relationships • Close/distance • Harmony/conflict • Abuse • Alliances • Health problems • Mental illness • Behavior problems • Legal problems • Substance abuse
Cynthia R. In-Home Therapist EcoMap Dr. Will Family Physician Janet S. Social Work Case Mgr Bill J. Probation Officer Rev. Jim P. Pastor Tim S. MH Therapist Verna H. School Counselor Geof G. School Soccer Coach
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 Age Continuous Timeline Series of school disciplinary actions for threats Fighting with peers Arrested for breaking into garage Mother enters AODA Tx Delinquent peers Burns down garage; shoots animals with pellet gun More defiant with teachers Joins Scouts but dismissed for stealing Shuttled between households Referred to school psychologist Mother & step father divorce Persistent lying Peer conflicts; fighting, stealing Poor reading comprehension & math; IEP Stuttering Start school; socially delayed, anxious, distractible Delayed toilet Child with extended family; foster family Child exposed to violent domestic abuse; child physical abuse Mother has series of brief abusive relationships; neglectful Birth mother 15; father abandoned; grandparents ashamed
Timeline by Age and Category Note: Use age ranges & categories that fit your client
Time & Factor Grid • How have these changed over time? (frequency, duration, intensity, pervasiveness; diagnoses, reactions & consequences, etc.) • Resources & constraints; strengths & weaknesses • Critical turning points • Blank areas of unavailable or insufficient information • Treatment history & response
Symptom Clustering Talks back to teachers Does not follow rules • Sources of information: • Interviews • Observation • Test results • Treatment records • Incident reports • Etc… Pushing, shoving, hitting Argues with adults Uses angry tone when responding Defies direction Irritability Loses or misplaces things Poor concentration Easily distractible Worry Disorganized Irritability Physical complaints Fidgets a lot Restlessness Careless mistakes Short attention span Sleep problems
Differential Diagnosis Steps Establish the boundary with no mental disorder (judgment whether it is clinically significant) Differentiate adjustment disorders from residual other specified/ unspecified disorders (symptoms present but below criteria may be due to adjustment to psychosocial stressor, or (un)specified reasons it does not meet criteria) Determine specific primary disorder(s) (see Section II of DSM-5 and differential diagnosis decision trees) Rule out disorder due to a general (e.g., nonpsychiatric) medical condition Rule out substance etiology (incl. drugs of abuse, medications and whether the use would present as mental disorder symptoms) Rule out malingering & factitious disorder (deceptive behavior due to some advantage) Symptom Presentation
FACES-1 Cohesion Disengaged Separated Connected Enmeshed Chaotically Disengaged Chaotically Enmeshed Rigid Structured Flexible Chaotic Adaptability Rigidly Disengaged Rigidly Enmeshed Olson’s Circumplex Model of Family Systems: FACES IV Balanced Families http://www.facesiv.com/home.html
Expected Outcome Actual Outcome Criticize the child Past criticism Poor grades Poor grades Child becomes angry & recalls past criticism Low esteem Criticize child for poor grades Wants to defy and frustrate parent Child’s behavior improves Too threated to react directly so is passive Past abuse Pressure by adults Preoccupied, anxious thinking
It really is very simple………….. You just have to pick a piece of it…
Sample Systems Diagram of Sex Offense Cycle 16, Rationalizes, “forgets” 1. Feels okay 2. Trigger event 3. Feel victimized, betrayed, helpless, abandoned & takes victim stance 15. Distracts self from discomfort, gets busy 4. Depressed, self- directed anger 14. Fear of getting caught, shame, guilt Revenge fantasy boring; thrill threshold higher 5. Withdraws, isolates 6. Revenge fantasies initially reduces tension 13. Feels re-empowered, relief, equilibrium Gets caught, feels victimized, recycles 7. Thinking errors justify revenge fantasies 12. Assault: sexual, physical, verbal 8. Act-out gets back at others 11. Victim grooming sets up opportunity to assault 9. Thinking errors justify act-outs 10. Self- destructive
Dad guilty about being on road; tries to rescue Mom Jane’s escalating mood, defiance Dad brings up long history of bad behavior & shaming Sample Family Cycle Mom cries, Dad escalates & threatens Jane Escalating conflict between Mom & Jane Jane runs out, desperate, angry Etc… Jane tests limits with teachers, Day Tx staff, etc. Jane persists in testing limits Numbing, dissociation, cuts to relieve Hospitalization, family shame Mother inconsistent in setting limits Mother overwhelmed with parenting, poor skills, low tolerance Family suppresses issues that build up
Mother’s subsystem of thoughts, feelings, experiences that lead to leniency Sample Family System Dynamics: It’s all tied together– treat the system! Father’s subsystem of thoughts, feelings, experiences that lead to strictness Son’s behavior issues Father’s Strict Truancy Parental conflict Mother’s leniency Frustration with school ADHD Verbal abuse Son observes Poor academic performance Physical abuse Angry about abuse Depressed, preoccupied about situation Referred for discipline Poor concentration at school Withdrawal by each Self- justification Hypersensitive, reactive Defiant with teacher Fighting with peers
Key elements Essential components of case conceptualization: • It tells a story: • identifying the key elements in a case (people, situations, behavior, internal processes, etc.) • how they are related to problem origin, • development of the problem, • maintenance of the problem (resistance to change), and • how it can be resolved (leverage points)
Criteria for selecting a leverage point: How do you decide where to intervene? • Most obvious • First presented (presenting problem) • Consensual (agreed on) • Where the pain is (most motivation) • Easiest to change (small wins) • Critical point (major issue) • Waterfall (affect next one) • Central (branch to other areas) • Available resources (time, skill, funding, etc.)
Force Field Analysis: How to get parents more engaged Forces for Change Barriers to Change Status Quo Disabled mother (meth) Supportive Father Long driving distance Family therapy rec. Reduce barriers rather than trying to increase drivers Child wants to see parents Parents “burned out” Parents resist meds Previous response ADHD meds 3 month funding Positive response to Tx Probation support Inactive DHS Case Mgr Relative strength of the factor
Amenability & fit Questions to determine Amenability & Fit— • Capacity level: Do limitations restrict being able to benefit from available treatment? • Motivational level: Is there sufficient belief in capacity, belief effort will be rewarded, and outcomes valued to benefit from available treatment? • Risk/safety factors: Are there significant risks that must be controlled for in the Tx environment? • Sanctions: Are there sufficient controls, restrictions, and consequences available to contain & motivate behavior? • Facilitating conditions: Are environmental and interpersonal supports available? • Barriers: For barriers to treatment, are there enhancers, substitutes and neutralizers available? • Feasibility: Given the above risks, requirements, and restrictions, can staff and facility provide appropriate treatment?
Watching a slow-motion accident: When there is no leverage point • Consult to check information, reasoning & options • Explore how resistances can be reduced • Move the intervention to a higher level of authority (e.g., child protection, courts) • Consider shifting to perspective taking and less emotional empathy • Prepare a safety net for the consequences • Understand how the “system” works to produce such a resistant situation
Good case conceptualization Characteristics of good case conceptualization • Identifies and utilizes key factors (people & events) in a comprehensive history & story • Accounts for origin, development, maintenance, resistance, and resolution of the problem • Shows relationships among key factors (causation, influence) • Plausible– makes sense without resorting to exceptional assumptions • Theory & Evidence-based– uses what is verified and documented by good sources, and there is a sound and appropriate framework for using the concepts for the case • Has implications for effective leverage points for intervention • Enables testing of the model– emerging information modifies the model
Clin process model Diagnostic & Treatment Process Treatment Cycle Purpose: Identify condition, treatment planning, research, insurance, regulation, eligibility, case management, best practices, etc. Diagnostic Cycle Diagnostic label Stage 4: Diagnosis Stage 3: Clinical Picture Case conceptualization: Story how the constructs are related based on best current evidence Intervention strategy: formulate goals & identify leverage points based on clinical description Stage 2: Identifying Constructs Psychological constructs: “anxiety, aggression, self esteem,” etc. Target behaviors and relationships Stage 1: Data Gathering Sources of raw data: observations, records & documents, test items, self and other reports, etc. Outcome measures & evidence
…and eventually… it all fits together into a picture of the client’s world and how it works
Q&A Whatdya mean, you want directions?