Download
1 / 26
260 likes | 337 Views
Extract: Protocol Design. STEMI < 6 h Lytic eligible. Lytic choice by MD (TNK, tPA, rPA, SK). ASA. Double-blind, double-dummy. ENOX < 75 y: 30 mg IV bolus SC 1.0 mg / kg q 12 h (Hosp DC) ≥ 75 y: No bolus SC 0.75 mg / kg q 12 h (Hosp DC ) CrCl < 30: 1.0 mg / kg q 24 h.

E N D
Extract: Protocol Design STEMI < 6 hLytic eligible Lytic choice by MD(TNK, tPA, rPA, SK) ASA Double-blind, double-dummy ENOX < 75 y: 30 mg IV bolus SC 1.0 mg / kg q 12 h (Hosp DC) ≥ 75 y: No bolusSC 0.75 mg / kg q 12 h (Hosp DC) CrCl< 30: 1.0 mg / kg q 24h UFH60 U / kg bolus (4000 U) Inf 12 U / kg / h (1000 U / h)Duration: at least 48 hCont’d at MD discretion Day 301° Efficacy Endpoint: Death or Nonfatal MI1° Safety Endpoint: TIMI Major Hemorrhage Antman EA et al. NEJM 2006;354
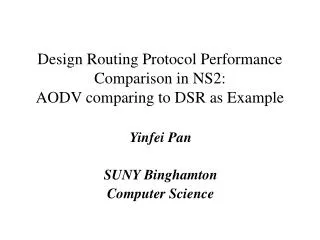
ExTRACT-TIMI 25: Primary End Point (ITT) Death or Nonfatal MI UFH 12.0% 17% RRR 9.9% Enoxaparin Primary End Point (%) Relative Risk0.83 (95% CI, 0.77 to 0.90)P<.001 Lost to follow-up = 3 Days after Randomization Adapted with permission from Antman EM, et al. N Engl J Med. 2006;354:1477-1488.
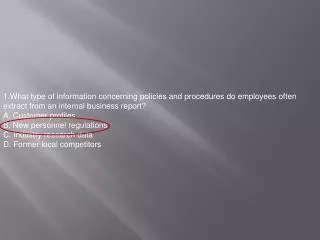
Bleeding Endpoints (TIMI) 30 Days UFH ENOX ARD 0.7%RR 1.53P<0.0001 ARD 0.4%RR 1.39P = 0.014 ARD 0.1%RR 1.27P = 0.14 % Events Major Bleed(fatal + nonfatal) NonfatalMajor Bleed ICH Antman EA et al. NEJM 2006;354
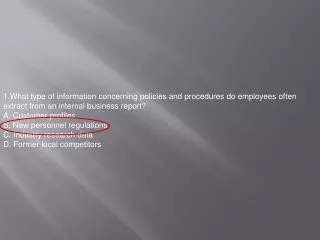
Major Hemorrhagic Events (Acute Phase) No significant increase in rate of major hemorrhage 60 Number of patients NS UFH Enoxaparin 40 NS NS 20 0 ESSENCE n = 3171 TIMI 11B n = 3910 TESSMA n = 7081 UFH, unfractionated heparin; NS, not significant Antman EM et al. Circulation 1999;100:1602-8
Severe / moderate hemorrhage Death or re-MI Abciximab + 7.4% 4.6% reteplase D = 2.3% P < 0.001 D = 1.4% P = 0.001 8.8% Reteplase 2.3% 6 4 2 0 2 4 6 8 10 Percentage of patients GUSTO V Benefit vs. risk GUSTO V Investigators. Lancet. 2001;357:1905.
Low-Molecular-Weight Heparin Advantages Disadvantages • Increased anti-Xa to anti-IIa activity inhibits thrombin generation more effectively • Induces ↑ release of TFPI vs UFH • Not neutralized by platelet factor 4 • Less binding to plasma proteins (eg, acute-phase reactant proteins) more consistent anticoagulation • Lower rate of HIT vs UFH • Lower fibrinogen levels • Easy to administer (SC administration) • Long history of clinical studies and experience, FDA-approved indications • Monitoring typically unnecessary • Indirect thrombin inhibitor • Less reversible • Difficult to monitor(no aPTT or ACT) • Renally cleared • Long half-life • Risk of HIT Hirsh J, et al. Circulation. 2001;103:2994-3018. TFPI = tissue factor pathway inhibitor; UFH = unfractionated heparin; SC = subcutaneous; aPTT = activated partial thromboplastin time; ACT = activated coagulation time.
IIa C AT IIa S Hep UFH Direct antithrombin AT Xa LMWH
Heparin fails to effectively inhibit Clot-bound Thrombin
Bivalirudin inhibits Clot-Bound and Circulating Thrombin
Bivalirudin: Unique mechanism of action overcomes the limitation of Heparin