Download
1 / 18
180 likes | 257 Views
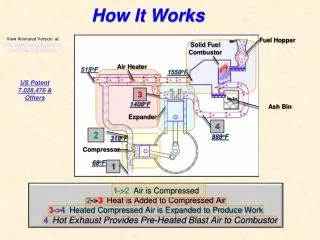
Mobilization in the Critical Care Unit (How It Works). Craig Moreland, PT, MS Director of Physical Therapy, UPMC Presbyterian, Montefiore, and Western Psychiatric Institute & Clinic Annual PM&R Assembly. The Physical Therapist’s Role in the ICU. 3 main goals:

E N D
Mobilization in the Critical Care Unit(How It Works) Craig Moreland, PT, MS Director of Physical Therapy, UPMC Presbyterian, Montefiore, and Western Psychiatric Institute & Clinic Annual PM&R Assembly
The Physical Therapist’s Role in the ICU • 3 main goals: • Optimize oxygen transport and the function of its supporting systems • Reduce multi-system complications • Maximize functional recovery and minimize diffuse atrophy
What we, as therapists, need to know… Basic cardiopulmonary pathophysiology Complications of bedrest and physiologic change associated with deconditioning Common ICU medications Emergency procedures Role of the other ICU team members All monitoring equipment Ventilator and respiratory equipment
The Physical Therapist Evaluation Previous Level of Function Mental Status Time of DIS (Daily Interruption of Sedation) Assessment of Lines, Tubes, and Drains
What We Need to Coordinate to Set Us Up to Succeed! • Timing is Everything!! • Medications (pain, anxiety) • Sedation Interruption • Weaning Trials • Respiratory Therapy • Occupational Therapy • Nursing
~The Mobility Team~ Physician Nursing Staff Pharmacist Occupational Therapist Speech Therapist Physical Therapist Respiratory Therapist Rehabilitation Aides
The Action! What Can We Do? Positioning Postural Drainage Cough Assist Splinting Exercise Transfer, ADL, and Balance Training Ambulation Education (invaluable)
Therapy ICU Intervention: Positioning and Postural Drainage: • Position the patient for respiratory success (eg. Anterior vs. Posterior Pelvic Tilt) • Postural drainage is accomplished by positioning the patient so that the position of the lung segment to be drained allows gravity to have its greatest effect • We to remember to write signs in the patient’s rooms to increase communication… • Patient is in semi-left-sidelying to drain the right middle lobe for 30-45 minutes for optimal respiratory mobilization; patient positioned at 10:30am
Therapy ICU Intervention Exercise: • Get Family Involved • Educate Nursing • Strengthen Respiratory Musculature • Primary: Diaphragm, Intercostals • Accessory: Sternocleidomastoid, Scalene
Therapy ICU Intervention Cough Assist: • Asthma Patient: ~teach a “pump cough” ~a forceful prolonged exhalation can lead to distress • COPD Patient: ~difficulty with expiration ~do not teach “take a deep breath” ~controlled small breaths • Neuromuscular Paralysis: ~maximize airway clearance ~make sure the patient can swallow safely ~position for success, couple extension & inhalation, couple flexion & exhalation
Therapy ICU Intervention Prior to initiating our mobility project, we needed to train all staff in… • Body Mechanics • Proper Lifting • Safety with Functional Transfers • Proper Guarding Techniques
Therapy ICU Intervention Transfer and Balance Training: • Monitor the Ventilator and Vital Signs • Blood Pressure with Change in Position • Transfers are the mainstay of our ICU treatment sessions • Who is doing what to ensure safety??? • ONE PERSON IN CHARGE • We always try incorporate quality of life into our treatment sessions!!
Who Does What? Setting Up the Room Scanning the Lines, Tubes, Drains Scanning the Ventilator Inspecting the Patient Who Holds What Line? What is each healthcare worker’s role?
Therapy ICU Intervention Ambulation is Our Ultimate Goal!! • Preparation • Multi-disciplinary Approach • Portable Ventilator Available? Education is Invaluable!! • Patient, Family Member, Health Care Team
Therapy ICU Intervention What Equipment will the mobility team need? • Ventilator, Ambu Bag, or Portable Oxygen • Portable Monitor or Pulse Oximeter • IV pole • Lines, tubes, drains • Assistive Devices • Chairs
When Does the Therapist Modify Activity??? FiO2 greater than 60% PEEP greater than 10 cm H20 pressure Consistent O2 Saturations less than 92% Hx of desaturations with positional changes Unstable Blood Pressure Severe Acidosis with pH less than 7.30 ~~~While many of these may not be absolute contraindications to mobilization, they should be cause to stop and discuss with the medical and nursing team prior to continuing~~~
Just Remember… ~~~The most important skill for a therapist to develop in the Critical Care Unit is to recognize when to initiate, delay, progress, and terminate treatment~~~