Download
1 / 55
740 likes | 961 Views
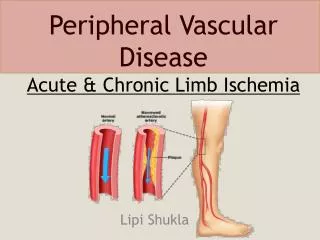
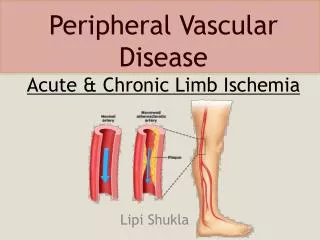
Acute Limb Ischemia. Acute Limb Ischemia:. sudden decrease in or worsening of limp perfusion causing a thread to extremity mobility and viability that has been present for less than 14 days. There is no time for collaterals to form.

E N D
Acute Limb Ischemia: • sudden decrease in or worsening of limp perfusion causing a thread to extremity mobility and viability that has been present for less than 14 days. • There is no time for collaterals to form. • may lead to irreversible tissue loss within hours if rapid diagnosis and restoration of flow are not achieved.
Etiology: • Embolism * (the most common) • Thrombsis • Trauma • Iatrogenic
Embolism • Translocation of material within the arterial stream to a more distal site. • 80% of the emboli are cardiac in origin • Or it may come from an Aneurysm • OrAtherosclerotic plaques. • Usually lodges at site of bifurication , most commonly the femoral artery . Sources of emboli:
Cardiac pathology. 80% • Atrial thrombus. (atrial fibrillation – atrial cardiac myxoma) • Ventricular thrombus. (following MI – ventricular aneurism) • Damaged valves . (RHD produce microemboli) • Patent foramen ovale. (allow paradoxical embolism to travel from venous into arterial circulation)
Proximal arterial pathology : (arterial –arterial embolism) • Aneurysm (most commonly the infrarenal aorta or popliteal arteries – may harbor a mural thrompus) • Atherosclerotic plaques. (serve as a nidus for thrombus or platelet aggregate that embolize distally – rupture discharging small debris.
In situ thrombosis: • Thrombosis of a chronically diseased vessel (most commonly SFA and popliteal A- may cause acute ischemia if collateral circulation is poorly developed ) • Hypercoagulable states .(even if the arterial segment is normal – generally occurs in the more distal segments such as tibial vessels or pedal arches)
Clinical presentation: • The “6 Ps” define this syndrome: • Paresthesias . The 1st to appear. (sever neural dysfunction –herald impending limp loss –an insensate limp is generally considered nonviable • Pain(acute onset – severe – unremitting-mainly unilateral ) • Pallor(associated with coolness – occurs at one level below the occlusion) • Poikilothermia(coldness). • Plusless( and usually will not have detectable Doppler signals distally because their collaterals may not be developed enough to support distal flow. • Paralysis(result as muscle function is severely compromised – heralds limp loss if blood flow is not restored promptly)
How to mange this patient: • History: • Pain: onset, location, duration • Hx of previous claudication • Hx of cardiac disease: valvular HD, atrial fibrillation, MI * (the commenestptn. of acute limb ischemia) ,cardiomyopathy • Hx of recent trauma • Risk factors of cardiovascular disease: (HTN – DM – hyperlipidemia – smoking – family history)
Physical examination: • Compare with contralateral extremity involving: • Level of pulslesness . • Temperature . • Mottling . • Motor and sensory examination • Cardiac Ex :rhythm , murmurs
Investigations: • Non invasive examinations: • Doppler signals . Other non invasive Ex generally are not performed at the interest of time. • Invasive procedures : - Arteriography : to define the level of occlusion and distal reconstitution.
Treatment : • Goals : rapid restoration of blood in order to save the limb , but not on expense of life. Strategies: • ABCs • Heparin: to prevent further propagation of the thrombus. • Thrombolytic therapy in selected patients. • Rapid surgical restoration(revascularaization) : thrombectomy.
Heparin therapy : initial therapy for patient with AAI, unless there is contraindication – 100 u/kg bolus then continued empirically at 1000 u/hr up to the time of surgery • Hydration :to maintain adequate urine output . Alklinazation of urine and osmotic diuresis are used to protect the kidney from damage by myoglobinuria in patient with prolonged sever ischemia
Revascularization : Definite treatment – ideally is performed within 6h of the onset to avoid irreparable nerve and muscle damage. Surgical therapy :the patient should be taken directly to OR following heparinization especially if motor and sensory changes are present. • Embolectomy (the procedure of choice for macroembolism to a large artery) • Bypass ( thrombosis – when adequate thromboembolectomy can not be performed)
Thrombolytic therapy: In selected patients such as those with prior vascular intervention. Tissue plasmiogen activator and urokinase have been used to dissolve acutely formed thrombus. Contraindications include : Prescience of sensory and motor changes on presentation (it requires 24h of treatment Recent surgery Known intracranial pathology
Complication of revascularization: Reperfusion injury, which has two effects: • local effect : compartment syndrome . For that reason ,fasciotomy is done with thrombectomy as prophylactic. • Systemic effect: release of K & myoglobin. This will lead to cardiac arrest & ARF.
Compartment syndrome: Reperfusion injery to the muscle may result in swelling and increased compartment pressure within the facial spaces of the calf . Pathophysiology: Endothelial cell injury during ischemia capillary permeability and edema Tissue swelling after reperfusion intracompartment pressure (more than capillary perfusion pressure – 30 mmhg) decrease perfusion Ischemia and myonecrosis
Clinical features: Pain :after passive movement of the foot Paralysis Parasthesia Pallor Pulse usualy present Diagnosis: History Suspicion Measuring compartment pressure
Management : • Prevention : low threshould for faciotomy • Treatment : opening compartments via bilateral calf incision
What is ulcer ? • Ulcer is a break through an epithelial surface .
Types of lower limb ulceration : Iatrogenic Bandaging ,Casts Neoplastic 2% BCC , SCC Melanoma Marjolin’s Lymphoedema Traumatic Vasculitic RA ,PAN Metabolic Pyodermagangrenosum Pretibialmyxoedema Cryopathic • Vascular *** • Venous 70% • Arterial 10% • Mixed 10% • Neuropathic • DM • Alcohol • Spina bifida • Infective • Fungal • TB • Syphilis • Leprosy
Venous ulcer : • The most common cause of leg ulceration is venous disease . • Two third of all leg ulcers are caused by venous disease. Pathophysiology: • Reflux (90%) • Obstruction (10%)
Pathophysiology: • Reflux of venous blood will lead to venous hypertention • This in turn leads to edema and leakage of blood cells and fibrin into the tissues • This will cause discoloration and hardening of the tissues (lipodermatoscelerosis) • These tissues are then prone to injury
Valvular incompetence resulting in reflux may occur in either : - spuerficial veins resulting in varicose veins , or - deep veins (e.g. DVT is a cause of deep vein incompetence)
Causes of obstruction : • Pregnancy • Fibroids/ovarian cysts • Abdominal lymphadenopathy • Pelvic cancer • Iliac vein thrombosis
Evaluation • History • Physical Examination • Investigations Non-invasive (Doppler/Duplex) Invasive ( Venography)
History • History : age , sex, occupation • History of leg ulcer : duration , No. of ulcers or episodes , pain, discharge • Vascular history: Hx of DVT, venous surgery, sclerotherapy , Hx of claudication and IHD, CVA ...
Examination Local : • The leg: varicose veins , arteries and nerves • the ulcer: site ( gaiter area = above the medial malleolus), shape , size, edge (sloping), base ( usually covered with granulation tissue, depth ( usually shallow), discharge. • the surrounding tissues : usually show signs of chronic venous hypertentsion – induration and pigmentation, warmth, redness, tenderness. General : examine the abdomen, the other leg , local lymph nodes
Investigations • Non-invasive : Doppler ( augmentation, phasic movement), ABI (Ankle-Brachial Index) Duplex ( compressibility, valve incompetence) • Invasive : venogram
Keys to management: • Elevation of Feet at right atrial level • Dressings • Compression • +/- surgery
Management • In patient with venous ulcer due to superficial incompetence varicose vein surgery is effective . • In deep venous incompetence : - local ulcer management - application of compression
Local ulcer management • Clean the ulcer by soaking it in tap water • Debride the ulcer to remove any slough • no role for topical antibiotics or topical drugs to speed the healing • The most important factor in achieving healing is the use of high levels of compression
Compression • Dressing alone is not enough • It has been found that pressures of 30-45 mmHg applied to the ulcer are much more effective than lower level of compression • These can be achieved by - Compression stocking or by bandaging ( e.g. four-layer bandaging technique)
Sclerotherapy, • endovenous laser therapy (EVLT), endovenous ablation therapy and • surgery are other option to treat the underlying cause.
Neuropathic ulcer • Occur over pressure areas • Usually are deep penetrating ulcers • The surrounding tissues are healthy and have a good circulation • Painless
Diabetic Neuropathic ulcer It result from a combination of factors • peripheral polyneuropathy • ischemic changes due to arterial disease • retardation of wound healing • infection
Management General measures : • control diabetes • stop smoking • lose weight • refer to chiropodist Local : • Treat infection with antibiotics • Antiseptic and dressings • Remove necrotic tissues • Amputations with debridement of dead tissues until healthy bleeding tissue is obtained
Malignant ulcers: • BCC • SCC • Melanoma • Marjolin’s