Download
1 / 23
230 likes | 526 Views
2. How do patients arrive at HES?. Outpatients (source of new referrals from Primary Care)GP (20% - mainly external eye)Optometrist (80%)Eye emergency (65% primary eye conditions)50% self-present 25% GP letter25% Optometrist letter Audits 2004-2006. 3. Current

E N D
1. 1
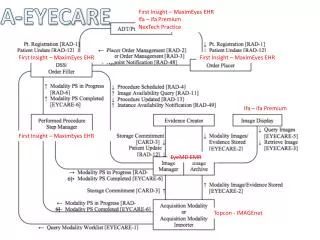
Eyecare pathways
David Parkins
Optometrist / PEC Commissioning (sec care)
2. 2 How do patients arrive at HES?
Outpatients (source of new referrals from Primary Care)
GP (20% - mainly external eye)
Optometrist (80%)
Eye emergency (65% primary eye conditions)
50% self-present
25% GP letter
25% Optometrist letter
Audits 2004-2006
3. 3 Current referral position
General Ophthalmic Services terms of service - Optom has duty to inform GP if signs of injury, disease or abnormality of the eye or elsewhere.
General Optical Council referral rules 1999 allowed Optometrist to manage certain eye conditions if within their scope of practice and expertise.
Not clear if referral required when same form (GOS18) can be used for information only.
HES bound to see patient.
4. 4 Referral decision making
Reasons why some patients are referred for further investigation can be related to the practitioner�s expertise, training or mode of practice.
As a result, some of the referrals do not require the expertise of a full consultant clinic appointment.
Referral decisions can often be refined in the practice but the NHS system does not fund this work, so the referral option may be the only alternative for some.
5. 5 Referral Data national average
4- 5%
6. 6 Referral data
26% of Bexley referrals came from 2 practitioners with referrals rates of 18% and 14% respectively (Audit 2005).
Audit 2006 � similar data � different practitioners.
Dry macular and pigmentary changes.
Confirmed view that the majority of inappropriate referrals can come from a small number of practitioners.
HES can therefore get a biased view of optometrist skills from the referrals it receives.
Not the true picture as more experienced practitioners do not show up on the HES radar.
7. 7 Result?
QMS over 65% of patients are discharged at 1st appointment.
250 new referrals per month
Issues over incomplete and inappropriate referrals (2001 audit - 57% practitioner could not be identified)
Referral quality = clinical confidence
8. 8 Ophthalmology pathway
Nothing to alleviate pressure of new referrals into system or provide continuity of care in primary care.
18 weeks target.
Need new ways of working and pathway redesign � ageing population and patients with long term conditions � diabetic retinopathy, glaucoma.
9. 9 Solutions
Clinical Assessment since Sept 2006 �
Issued referral guidance Oct 2006
covers Glaucoma, Diabetes, ARMD & Cataract - 80% of referrals
Feedback on quality of referral, training and development issues
Support for practitioners
10. 10 Referral Guidance
11. 11 Glaucoma Potentially blinding disorder requiring life long care once diagnosis is made.
Prevalence 2% of the >40s to 10% of the >70s
Approx 50% already detected
HES 33% discharged, 33% suspect, 33% confirmed (RNIB)
High prevalence of false positives due to low prevalence of undetected cases.
However, number of false positives can be decreased by repeat testing, but optometrists are not funded by GOS to do so.
12. 12 Glaucoma Audit Jan 05 identified 60% of glaucoma referrals required more information - all 3 tests
Scan of anonymised referral removed � copied for information
R +4.00/-0.50 x 80 6/5 L +3.75/0.25 x 110 6/5 +1.75
NO disc assessment
NO visual field assessment
IOP by NCT RE 24, 23 LE 25, 25
Mrs XXXXX has high pressures. Given that her father has glaucoma, please refer to be examined by a consultant.
13. 13 Glaucoma refinement Under tariff, high false positive rate becomes an issue.
Introduced refinement scheme � July 05.
Before the decision to refer is made, if a patient with suspect fields and pressures meets criteria, they can be seen again on another day for repeat fields (by the optometrist) and/or applanation tonometry (by the optometrist).
Encourages improved quality of referral = all 3 tests
Glaucoma referrals reduced by 43%.
Saving an unnecessary referral and undue worry to patient.
14. 14 Glaucoma shared care Eye care pathway pilot
Peterborough scheme reported
Using accredited optometrists to co-manage and monitor glaucoma patients is a viable alternative strategy.
Needs more work to determine if cost effective model in optometric practice.
Alternative models could take place in HES or community practice site if space and equipment available.
15. 15 Diabetic screening
NICE guidelines � examine eyes at time of diagnosis and at least annually.
NSF set a target of 100% being offered screening by the end of 2007 � currently less than 50% receiving SL BIO screening locally.
Digital imaging photography � hard record
New scheme requires a high standard of QA
Current SL- BIO scheme ceases at the end of 2006
Four camera sites � in Optometric practice.
Central patient database and recall centre
Patients on register will be sent annual appointments
VA�s, dilation, photos, grading of images
SL- BIO for ungradeable images � eg cataract
16. 16 Diabetic Screening Optometrists who see patients with diabetes (or glaucoma) under the GOS have a duty to notify the GP of their findings.
If patient not under any screening review - advice will be for Optom to inform GP.
Any decision to refer for retinopathy by community Optoms will depend on H&S and time since last screening.
New gradings for camera scheme R0, R1 - annual screen.
R2, M1 - 13 weeks R3 - 2 weeks
Likely to be an increase in secondary referrals due to previously unknown pathology detected on images.
17. 17 Macular degeneration (ARMD) Dry
Signs: drusen and focal pigmentary changes
Gradual deterioration in VA
Some optometrists refer to protect themselves
No treatment � increased reading additions, magnifiers
Advice � lighting, diet, stop smoking.
Amsler grid to monitor.
Do not usually require referral if asymptomatic, except for LVA�s, other co-morbidity eg cataract and finally registration.
18. 18 Treatable ARMD Wet
Recent onset of symptoms � distortion scotoma, shadow or patch in central vision.
Referral criteria for PDT:-
VA 6/60 or better in the affected eye
Recent sudden onset of central distortion
Fundal appearance suggestive of choriodal neovascularisation
FAX urgent referral to Kings College � to be seen within 2 weeks.
19. 19 Cataract C&B Pathway
Issued cataract referral guidance 2006
Cataract C&B through NHS Direct ceases end of year due to loss of SHA funding.
Bexley booking model � as from Jan 2007
After dilated assessment by optometrist, referral is faxed to a central booking service where it is entered on C&B software and patient receives directions to complete booking with hospital of their choice.
20. 20 Cataract C&B Pathway Fax referral proforma automatically received in scan form by CBS.
Referral assessed for completeness (if appropriate continue with booking process. If not, sent back to optometrist to complete)
Patient located on Choose and Book software
CBS auto-generates password and creates UBRN and appointment request on Choose & Book software within a maximum of 2 working days of acceptance of the referral proforma.
CBS sends booking information letter, appointment request, UBRN and password to patient to allow them to complete booking with the hospital of their Choice.
CBS electronically attaches referral proforma scan to appointment request on Choose & Book software.
CBS sends confirmation to GP and Optometrist when appointment is booked.
CBS contacts optometrist and GP if patient fails to complete their booking.
21. 21 Cataract
22. 22 Children
NSF states that children aged 4/5years should be assessed on school entry.
No further screening checks thereafter.
Provision for free checks under GOS until 16 years, or under 19 years if still in FT education.
QMS Orthoptists trained school nurses to conduct basic eye screening.
Referral options either to Optometrist if suspect refractive problem or fast track Optom/orthoptist clinic if 2 lines difference in VA.
23. 23 CAS for time being so that pathway actively filtered by OPwSI�s - GP option to scan referrals onto nhs.net
OPwSI�s to see selected patients in the community to focus on reducing false positive referrals
Feedback to community Optometrist where appropriate.
Maintain strong links between local eye department and Bexley CT � important with increased Choice.
18 week target � identify further opportunities for joint primary/sec care pathway working.
24. 24 New eyecare groups will need to ensure whole pathway working by
The right people
Doing the right things
In the right order
At the right time
In the right place
With the right outcome
All with attention to the patient experience