Download
1 / 27
1.14k likes | 10.01k Views
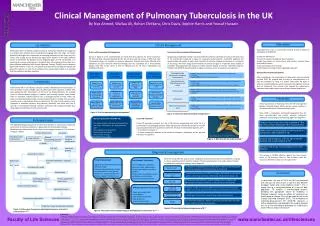
PULMONARY TUBERCULOSIS. By Dr. Abdelaty Shawky Assistant professor of pathology. * Definition: chronic infective granuloma affecting nearly all body systems but mainly the lungs . * Predisposing factors : a) Environmental: low socioeconomic level, bad general hygiene, overcrowding .

E N D
PULMONARY TUBERCULOSIS ByDr. Abdelaty ShawkyAssistant professor of pathology
* Definition: chronic infective granuloma affecting nearly all body systems but mainly the lungs. * Predisposing factors: a) Environmental: low socioeconomic level, bad general hygiene, overcrowding. b) Personal factors: cases of low resistance e.g. malnutrition – AIDS - D.M.
* Causative Agents:T.B. bacilli * Structure o f T.B. bacilli: Tuberculoprotein core covered by glycolipid. * Types of TB Bacilli: • Human type: transmitted from human to human by droplet infection. • Bovine type: transmitted from cows to human by ingestion of infected milk.
* Types of T.B: • Primary (1ry) T.B. • Secondary (2ry) T.B.
Primary tuberculosis(childhood type) * Age: - Occurs in young persons < 3 years, who are: non immunized, and infected for the first time. * Sites: • Lung. • Nose. 2. Intestine. 3. Tonsil. 4. Skin.
* Methods of infection: 1. Inhalation 2. Ingestion 3. Direct contact. * Tissue reaction (Reaction of the body against T.B bacilli): proliferative (tubercle formation).
*Pathogenesis of tubercle (T.B granuloma) formation: A. In the first 24 hours: • Carbohydrate coat of the bacilli recruits neutrophils, which fails to kill it. • Bacilli are taken by surface macrophages to the deep parts of the tissues, draining lymphatics & L.Ns. • Macrophages process the bacilli releasing the purified protein derivative PPD, then express it on the surface carried on MHC class II molecules.
B. After 10-15 days: - T.B granuloma is formed as follow; • Macrophages secrete IL-12 which activate the naïve CD+4 T lymphocytes to T helper (TH1) cells. • TH1 cells release lymphokines: 1. INF-y (interferon Gama) leads to macrophage activation. 2. IL-2 (interleukin-2) leads to lymphocyte proliferation. 3. TNF (tumor necrosis factor) & lymphotoxins
The accumulated macrophages undergo a morphologic transformation into epitheial-like cells (epithelioid cells). Some epithelioid cells coalesce to each other to form langhan’s giant cells. Collections of epithelioid cells, langhans giant cells and a collar of lymphocytes is termed (non-caseating tubercle).
C. After 2-3 weeks: • The tubercles undergo central caseation necrosis (very rare with 1ry T.B), the causes are: 1. Relative central ischemia. 2. Lymphotoxins. 3. Proteolytic enzymes of neutrophils.
* Gross picture of tubercle: Small, 1-3 mm, with central yellow caseation and grey periphery. * Microscopic picture of tubercle: Central caseating material (structureless, eosinophilic material, epithelioid cells, macrophages, Langhan’s giant cells, lymphocytes and peripheral fibroblastic reaction.
Lung is a favorable site for T.B. (easy inhalation and aeration). Types: • 1ry pulmonary T.B. • 2ry pulmonary T.B.
* Age: • Children. * Mode of infection: • Droplet infection. * Lesions: • More in the right lung than the left lung. • 1ry pulomnary complex (Ghon’s triad).
Primary pulmonary complex (Ghon’s triad) Consists of 3 parts: • Parenchymatous lesion (Ghon’s focus): - Tubercles which develop at the lower parts of upper lung lobes or upper parts of lower lung lobes, subpleural. - Consists of non-caseating and caseating tubercles. • Tuberculous lymphangitis. • Tuberculous lymphadenitis.
* Fate: A. Good fate: - Healing by fibrosis and dystrophic calcification. - Formation of a dormant T.B focus. B. Bad fate: Spread. • Local. • Lymphatic. • Hematogenous • Natural passage: through the lumen of bronchi
* Age: adults who are infected or vaccinated before. * Mode of Infection: • Reactivation of dormant focus. • Exogenous by inhalation. * Lesions: • It is only caseating tuberclous reaction (Assman’s focus or Simon’s focus) develop at the apical portion of the lung. • No complex formation.
* The Fate of 2ry pulmonary T.B: A. Good fate: - Regression and healing. In cases of good immunity. B. Bad Fate: - Progression and spread in cases of poor immunity. 1. Cavitary Tuberculosis 2. Chronic fibrocaseous pulmonary tuberculosis 3. Acute tuberculous bronchopneumonia & acute caseous pneumonia.