Download
1 / 53
570 likes | 1.65k Views
Therapeutic Drug Monitoring and penicillin allergy (Duty of care with toxic drugs). Dr Kieran Hand Consultant Pharmacist, Anti-infectives SUHT, November 2007. Why monitor drug levels?. Optimise dose regimen for individual patient Explain lack of efficacy Prevent / confirm toxicity

E N D
Therapeutic Drug Monitoring and penicillin allergy(Duty of care with toxic drugs) Dr Kieran Hand Consultant Pharmacist, Anti-infectives SUHT, November 2007
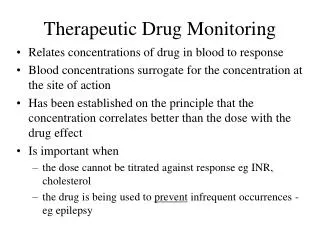
Why monitor drug levels? • Optimise dose regimen for individual patient • Explain lack of efficacy • Prevent / confirm toxicity • Evaluate impact of drug interactions • Evaluate impact of low albumin • Evaluate impact of changes in organ function or fluid status • Check patient compliance
Anti-epileptics Phenytoin, Carbamazepine, (Valproate) Antibiotics Gentamicin, Tobramycin Vancomycin, Teicoplanin Anti-psychotics Lithium Cardiac glycosides Digoxin Bronchodilators Aminophylline Theophylline Specialty drugs Drugs routinely monitored
Phenytoin – key points • Saturable metabolism so increase dose carefully • Long half-life (1 day) so pointless to sample blood before one week if initiating oral therapy • Serum levels must be adjusted for abnormal albumin concentration – call a pharmacist (low albumin leads to plasma phenytoin level appearing low but tissue levels normal) • Susceptible to protein binding displacement (plasma level appears low but tissue levels normal) • Susceptible to liver enzyme inhibition and induction
Carbamazepine – key points • Autoinduces it’s own metabolism (one month) • Wider therapeutic index than phenytoin • Susceptible to liver enzyme induction or inhibition • Induces increased metabolism of other drugs
Gentamicin extended interval dosing Concentration Time
Reduced elimination MTC Concentration MEC Time
Reduced elimination MTC Concentration MEC Time
Gentamicin – key points • Gentamicin causes permanent renal failure if levels are kept above 1mg/L for a prolonged period of time • High-dose regimen (5mg/kg) equally effective as traditional dosing • High-dose regimen no more toxic than traditional dosing • See SUHTranet for exclusion criteria
Vancomycin – key points • Activity related to time levels are above MIC for target pathogen • Vancomycin is rarely nephrotoxic if monitored carefully • Nephrotoxicity is usually associated with concurrent prescribing of other nephrotoxic drugs • ICU uses continuous infusion vancomycin
Teicoplanin – key points • Inferior efficacy to vancomycin • Frequently underdosed – associated with treatment failure • Levels sent off to Bristol - delay • Advantage of once-daily dosing • Reduce dose on 4th day if renal impairment • Less nephrotoxic than vancomycin • Expensive
Digoxin - key points • Low potassium potentiates risk of arrhythmias • Maintenance dose usually guesstimated from weight and renal function • Pharmacist can provide more accurate estimate • Clinically significant interaction with amiodarone • Digibind® reduces mortality in overdose but phenytoin is a cheaper alternative in mild cases
Lithium – key points • Renal excretion • 100% filtered but 80% reabsorbed • Li+ reabsorption linked to Na+ reabsorption • Influenced by dehydration, sodium depletion, hypotension • Diuretics (e.g. thiazides) can increase Lithium levels dramatically • NSAIDs and ACEi’s can increase Li+ levels toxicity
Theophylline / aminophylline key points • Theophylline concentration is increased in • Heart failure • Cirrhosis • Elderly • Liver enzyme inhibitors • Theophylline concentration is decreased by • Smoking • Social drinking • Liver enzyme inducers
Specialty drugs for monitoring – seek expert advice • Immunosuppressants • Ciclosporin / Tacrolimus / Sirolimus • Methotrexate • Anti-epileptics • Valproate • Phenobarbitol • Ethosuximide • Tricyclic antidepressants • Amitriptyline, nortriptyline, imipramine etc
Important concepts • You prescribe a toxic drug – you monitor it • Seek advice from the ward pharmacist or Medicines Info • Loading dose for drugs with long half-life • Distribution phase (when to sample blood after dose given) • Documenting sampling times • Steady state (when to check levels after start of therapy or change to therapy) • Actions: reducing dose or extending dosing interval • Slow-release brands are not easily interchangeable • Many TDM drugs are susceptible to serious drug interactions – caution if starting/stopping other drugs and check with pharmacist or BNF
Penicillin allergy • Megan, 19-years-old, student • PC ‘Serious infection’ • Allergies ‘Penicillin – itchy rash and lips swollen’ • Rate the following antibiotics as: • Safe • Caution – perform risk assessment • Danger
Clindamycin Amoxicillin Moxifloxacin Daptomycin Doxycycline Tazocin Azithromycin Gentamicin Metronidazole Ceftriaxone Vancomycin Flucloxacillin Meropenem Cefuroxime Augmentin Rifampicin Penicillin allergy
Clindamycin Amoxicillin Moxifloxacin Daptomycin Doxycycline Tazocin Azithromycin Gentamicin Metronidazole Ceftriaxone Vancomycin Flucloxacillin Meropenem Cefuroxime Augmentin Rifampicin Penicillin allergy
10-20% of patients reporting a penicillin allergy are truly allergic (Salkind 2001 JAMA) Frequency of all ADRs to penicillin in general population is 0.7-10% Anaphylaxis occurs in between 1:6,500 and 1:25,000 penicillin courses History of atopy is not predictive of penicillin anaphylaxis but may severity Patients on beta-blockers may be at increased risk of death if anaphylaxis occurs Understanding the classification of penicillin hypersensitivity reactions helps with risk assessment Facts about penicillin allergy