Download
1 / 56
590 likes | 785 Views
PHYSIOLOGY: Digestion , Absorption & Defecation. Reference. Guyton A., and Hall, J. Textbook of Medical Physiology. 12 th ed. Seeley, R., Stephens, T., and Tate, P., Anatomy & Physiology. 8 th ed. McGraw Hill Company Inc., (2008). Functions of the Digestive System. Motility Functions

E N D
Reference • Guyton A., and Hall, J. Textbook of Medical Physiology. 12thed. • Seeley, R., Stephens, T., and Tate, P., Anatomy & Physiology. 8th ed. McGraw Hill Company Inc., (2008)
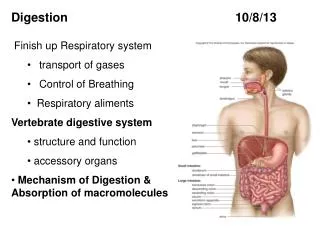
Functions of the Digestive System • Motility Functions • Propulsion • Mechanical Digestion • Secretory Functions • Chemical Digestion • Regulation • Absorptive Functions
Six basic processes are involved: ingestion, secretion, propulsion, digestion, absorption and defecation. Ingestion is taking food into the mouth. Secretion is the act of expelling a liquid. The cells lining the GI tract secrete about 9 liters (9.5 quarts) of water, acid, buffers, and enzymes each day to lubricate the canal and aid in the process of digestion.
Propulsion consists of alternating contraction and relaxation of smooth muscle in the walls of the GI tract to squeeze food downwards.
Digestion has two parts, mechanical and chemical. Mechanical digestionis chewing up the food and your stomach and smooth intestine churning the food Chemical digestion is the work the enzymes do when breaking large carbohydrate, lipid, protein and nucleic acid molecules down into their subcomponents -these and others are the nutrients.
Absorption occurs in the digestive system when the nutrients move from the gastrointestinal tract to the blood or lymph. Defecationthe act or process by which solid or semisolid waste material (feces) from the digestive tract are eliminated via the anus.
Digestion in the Mouth • Mechanical Digestion • Mastication reflex • Food enters mouth • Relaxation of muscles of mastication • Stretch reflex causes contraction
Digestion in the Mouth • Chemical Digestion by Saliva • Serous secretion for digestion of starches: amylase • Mucous secretion for lubrication
Swallowing • Oral • Pharyngeal • Esophageal
DEGLUTITION (SWALLOWING) accomplishes the propulsion of ingested food the mouth to the stomach. Three stages: Buccal Pharyngeal Esophageal
BUCCAL STAGE tongue moves upward and backward to push the food toward the pharynx. PHARYNGEAL STAGE coordinated involuntary actions which direct food to the esophagus closing the airway passages
ESOPHAGEAL STAGE peristaltic waves propel food from the esophagus to the stomach
NO Digestion in the Esophagus • No actual digestion • Propulsion via peristalsis • Mucous secretion for lubrication
Digestion in the Stomach • Food storage in the fundus • LES prevent reflux of stomach contents • Mechanical Digestion via segmental contractions • No absorption
Digestion in the Stomach • Chemical digestion by Oxyntic cell secretion
Chemical Digestion by Pancreas • Acini cells secrete pancreatic digestive enzymes into the hepatopancreatic duct to empty into the small intestine • Enzymes are not activated until they are mixed with acidic chyme
Biliary Secretions by the Liver & Gall Bladder • For fat digestion & absorption • Emulsify large particles for more efficient lipase action • Ease of absorption • Means of excretion of waste • bilirubin
Biliary Secretions by the Liver & Gall Bladder • Liver constantly produces bile and is concentrated in the gall bladder • Biliary secretions include HCO3- to neutralize the acidic chyme
Digestion & Absorption in the Small Intestine • Dominating chemical digestion via • Pancreatic secretions • Biliary secretions • Intestinal secretions
Digestion & Absorption in the Small Intestine • Absorption via transport processes • Water: diffusion through tight junctions • Carbohydrates: Na-Glucose cotransport; fructose via facilitated diffusion
Digestion & Absorption in the Small Intestine • Absorption via transport processes • Lipids: diffusion with bile salts • Proteins: Na-Glucose cotransport or endocytosis
Digestion & Absorption in the Small Intestine • Absorption via transport processes • Na: diffusion down a electrical gradient • Cl: diffusion via solvent drag • HCO3-: indirectly by secretion of H+ • *Other ions & vitamins are also absorbed
Absorption in the Large Intestine • Absorption of electrolytes occur but backflow is prevented by tight junctions • Water follows as result of osmotic gradient • Secretion of mucus for lubrication
Mouth -chewing & lubrication (saliva) Esophagus-conduit Stomach-digestion takes place -secretes pepsin + HCl Small intestine-duodenum jejunum ileum (functional reserve) Large intestine-stores and concentrates undigested material - colon: 3 limbs -ascending transverse descending
Rectum ampulla • temporary storage for waste. As the rectal walls expand, stretch receptors from the nervous system located in the rectal walls stimulate the desire to defecate.
Colon innervation: Intrinsic • Auerbach plexus- segmentation and peristalsis • Plexus of Meissner- secretions and sensation Extrinsic • Parasympathetic increases and relaxes sphincters • Sympathetic decreases motility and contracts sphincters
The muscular wall of the cecum and colon is innervated by: Vagus nerve- cranial nerve X in PNS Superior mesenteric plexus – SNS cord segment T9-L2 The rectum and anal canal innervation: Pelvic splanchnic nerves- parasympathetic S2-4 Hypogastric nerve- sympathetic T11-L2
Anal sphincters innervation: Internal anal sphincter- pelvic splanchnic nerves and hypogastric nerves External anal sphincter – pudendal nerve
Defecation Reflex • Integrated in the sacral region of the spinal cord • Stimulated by distention of the rectal wall • Weak contractions of rectal wall • Relaxation of anal sphincter
Defecation Reflex • May be inhibited by voluntary constriction of external anal sphincter
If the urge is not acted upon, the material in the rectum is often returned to the colon where more water is absorbed. If defecation is delayed for a prolonged period the fecal matter may harden, resulting in constipation.
During defecation the chest muscles, diaphragm, abdominal wall muscles, and pelvic diaphragm all exert pressure on the digestive tract and ventilation temporarily ceases as the lungs push the chest diaphragm down in order to exert pressure. Blood pressure rises. Not good for high- risk cardiac patients.
For defecation external anal sphincter must relax. Sphincter aniexternus muscle for anal and urethral are both closely linked by the same nerves
Fecal incontinence is the inability to control one's bowels. When one feels the urge to have a bowel movement, they may not be able to hold it until they can get to a toilet, or stool may leak from the rectum unexpectedly.
Fecal incontinence may be caused by physical injury (such as damage to the anal sphincter that may result from an episiotomy) intense fright, inflammatory bowel disease, impaired water absorption (diarrhea), and psychological or neurological factors.
BEFORE DEFECATION Fecal material passes to rectum by the longitudinal muscular contraction. When there is distension in the sigmoid colon and rectum, the internal sphincter relaxes at the same time as the external sphincter contracts. This allows some of the fecal contents to enter the anal canal and be sampled by its sensitive epithelium to determine if its solid, liquid or gas.
If the individual decides to continue with defecation, the intrarectal pressure increases on straining. Added pressure from abdominal straining orValsalva maneuver aids defecation. Straining requires intact innervation of the lower thoracic cord T6-T12. The pressure should be sufficient to overcome the external sphincter which relaxes with the pelvic floor that causing the rectum to straighten up reducing the rectal angle.
This increase in intraabdominal pressure forces stool into the rectum with relaxation of the extenal anal sphincter allowing defecation. Fecal matter stimulate the anal canal further relaxing the external anal sphincter.
If the individual decides not to continue with defecation, the rectum relaxes further to allow accommodation of the contents which further stimulates the external sphincter to contract.
Upper motor neuron lesion- damage above the defecation reflex center in the sacral cord Results to: • Abnormal storage of feces • Inability to recognize urge and distinguish contents • External sphincter dyssynergia