Download
1 / 36
520 likes | 848 Views
Cerebellum. Tim McDowell January 26, 2011. Anatomy. Midline vermis + 2 cerebellar hemispheres Anterior (I-V) and posterior (VI-IX) lobes divided by primary fissure Flocculonodular lobe (X), seperated by posterolateral fissures Cortex folded into folia. Anatomy. Deep Nuclei. Fastigial

E N D
Cerebellum Tim McDowell January 26, 2011
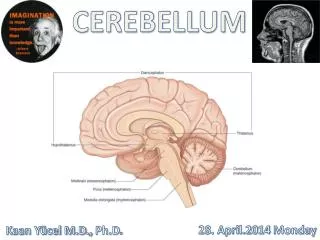
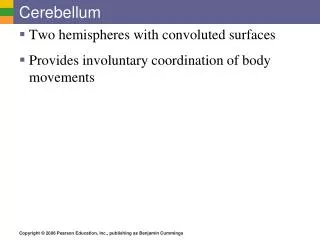
Anatomy • Midline vermis + 2 cerebellar hemispheres • Anterior (I-V) and posterior (VI-IX) lobes divided by primary fissure • Flocculonodular lobe (X), seperated by posterolateral fissures • Cortex folded into folia
Deep Nuclei • Fastigial • stance and gait, controls muscles only in the modes of sitting, standing, and walking • Globose + Emboliform • segmental reflexes, speeds the initiation of movements triggered by somatosensory cues that guide the response, stops unwanted and promotes wanted oscillations, stabilizes holds • Dentate • Fine dexterity
Functional Anatomy • Archicerebellum • flocculonodular lobe • connections with the vestibular system, inputs from areas of the brain concerned with eye movements • Paleocerebellum • vermis of the anterior lobe, the pyramis, the uvula, and the paraflocculus • Spinal cord inputs, controls muscle tone + axial and limb movements
Functional Anatomy • Neocerebellum • middle portion of the vermis and most of the cerebellar hemispheres • planning and initiation of movements, regulation of fine limb movements
Functional Anatomy • Organized into Midline, Intermediate and lateral zones • Midline project to fastigial nuclei • Intermmediate project to nucleus interposed • Lateral project to dentate
Cerebeller Cortex • 3 Layers: • Granular • Purkinje • Molecular • 5 Cell types: • Basket, stellate, Purkinje, granule, and Golgi
Physiology Ascending Fibres: • Mossy • Diffuse projections through granule cells to multiple Purkinje cells • Climbing • Terminal fibers of olivocerebellar tracts, multiple synaptic contacts per Purkinje cell • Multilayered • Afferents from hypothalamus, raphe n, locus ceruleus
Physiology Descending Fibres: • Purkinje Fibres • Project from Purkinje cells in Purkinje layer to deep cerebellar nuclei, inhibitory • Deep nuclei then send excitory signals to their efferent connections
Physiology • Stellate cells and basket cells cause lateral inhibition of Purkinje cells • Modulation in spatial resolution • Golgi cells inhibit granular cells • Modulation in temporal resolution
Afferent and Efferents • Superior Cerebellar Peduncle (brachium conjunctivum) • Connects with midbrain • Middle Cerebellar Peduncle (brachium pontis) • Connects with pons • Inferior Cerebellar Peduncle (restiform body) • Connects with medulla
Superior Cerebellar Peduncle • Afferent: • Ventral spinocerebellar tract, transmits proprioceptive and exteroceptive information from levels below the midthoracic cord. • Tectocerebellar tract, arising in the superior and inferior colliculi • carries auditory and visual information. • Trigeminocerebellar tract, proprioceptive fibers from the mesencephalon and tactile information from the chief sensory nucleus of the trigeminal nerve • The cerulocerebellar tract, fibers from the nucleus ceruleus
Superior Cerebellar Peduncle Efferent: (most prominent) • Dentatorubral tract, output to the contralateral red nucleus • Dentatothalamic tract, output to the contralateral ventrolateral nucleus of the thalamus • Uncinate bundle of Russell, output to the vestibular nuclei and reticular formation
Middle Cerebellar Peduncle • Afferent fibers: (only) • Pontocerebellar (corticopontocerebellar) tract, arises in contralateral pontine gray matter • Transmits impulses from the cerebral cortex to the intermediate and lateral zones of the cerebellum
Inferior Cerebellar Peduncle Afferent: • Dorsal spinocerebellar tract, originating in the dorsal nucleus of Clarke (T1–L2), carries proprioceptive and exteroceptive information mostly from the trunk and ipsilateral lower extremity • Cuneocerebellar tract, originating in the external arcuate nucleus, which transmits proprioceptive information from the upper extremity and neck. • Olivocerebellar tract, which carries somatosensory information from the contralateral inferior olivary nuclei.
Inferior Cerebellar Peduncle • Vestibulocerebellar tract, transmits information from vestibular receptors on both sides of the body. • Reticulocerebellar tract, arises in the lateral reticular and paramedian nuclei of the medulla. • Arcuatocerebellar tract, arises from the arcuate nuclei of the medulla oblongata. • Trigeminocerebellar tract, arises from the spinal and main sensory nuclei of the trigeminal nerve Efferent: • fastigiobulbar tract -(through Juxtarestifrom body), cerebellovistibular • cerebelloreticular pathways
Vascular Supply • PICA • From intracranial vertebral artery, supplies the lateral medullary tegmentum, inferior cerebellar peduncle, the ipsilateral portion of the inferior vermis, and the inferior surface of the cerebellar hemisphere • Medial branch supplies dorsolateral medulla and medial cerebellum, lateral branch supplies inferiopostalateral
Vascular Supply • AICA • above the origin of the basilar artery, supplies the anterior petrosal surface of the cerebellar hemisphere, flocculus, lower portion of the middle cerebellar peduncle, and lateral pontomedullary tegmentum • SCA • distal segment of the basilar artery just below the terminal bifurcation into the paired PCAs, and supplies the upper surface of the cerebellar hemisphere, ipsilateral portion of the superior vermis, most of the dentate nucleus, upper portion of the middle cerebellar peduncle, superior cerebellar peduncle, and lateral pontine tegmentum
Stroke Syndromes • PICA (40%) • Proximal (usually in vertebral arteries) • Wallenberg syndrome • Distal: • Medial branch occlusion will cause acute vertigo and truncal ataxia • Lateral branch occlusion :unsteadiness, limb ataxia, and dysmetria without dysarthria
Stroke Syndromes AICA (5%) • Prominent vertigo, nausea, vomiting, and nystagmus (vestibular nuclei) • Ipsilateral facial hypalgesia and thermoanesthesia, and corneal hypesthesia (trigeminal spinal nucleus and tract) • Ipsilateral Horner syndrome • Contralateral trunk and extremity hypalgesia and thermoanesthesia (lateral spinothalamic tract). • Ipsilateral ataxia and asynergia (middle cerebellar peduncle and cerebellum). • Ipsilateral deafness and facial paralysis (lateral pontomedullary tegmentum).
Stroke Syndromes SCA (35%) • Vertigo and vomiting (vestibular nuclei and connections) • Nystagmus (MLF and cerebellar pathways) • Ipsilateral Horner syndrome • Ipsilateral ataxia and asynergia (superior cerebellar peduncle and cerebellum) • Ipsilateral intention tremor (dentate nucleus and superior cerebellar peduncle) • Contralateral trunk and extremity hypalgesia and thermoanesthesia (lateral spinothalamic) • Contralateral hearing impairment (crossed fibers of the lateral lemniscus) • Contralateral fourth nerve palsy (pontine tectum)
Stroke Syndromes • Watershed (20%) • Etiologies: focal hypoperfusion secondary to occlusive disease in vertibobasilar vessels, emboli, intercranial atheroma, global hypoperfusion • Physical findings variable
Stroke Syndromes • PICA vs SCA • SCA has less frequent vertigo and H/A, both with gait disturbance • SCA typically more benign clinically • Always need to be aware of possible herniation (tonsillar or transtentorial) with cerebellar stroke
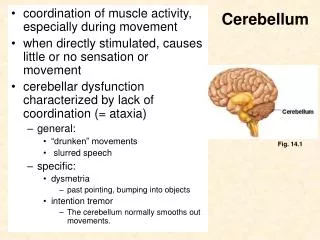
Clinical Features • Ataxia • Dysmetria, dysdiadokinesis, rebound, truncal, gait, localization dependent • Hypotonia, pendular reflexes • neocerebellum • Intention Tremor • Dentate nucleus, rubro-olivo-cerebellar circuit
Clinical Features • Dysarthria • Scanning speech, agrammatism, involovemnet of tongue representation in cerebellum (L paravermal) • Nystagmus • PAN, Rebound, Gaze evoked, downbeat (post. midline) • Abnormal Saccades • Square-wave jerks, macro square-wave jerks • Occular dysmetria • Difficult to localize eye movement abnormalities between cerebellum and brainstem
Video Cases SCA6 is a relatively “pure” cerebellar ataxia that usually begins in midlife. Many cases are sporadic, ie, occur in the absence of a known family history. In addition to describing so well her disease onset, progression, and current symptoms, this patient relates how it became clear, in retrospect, that her mother’s gait problems and cerebellar disease were not due to chemotherapy, as had been assumed. The examination illustrates common features of SCA6, including scanning dysarthria, end-gaze nystagmus, and gait ataxia greater than appendicular ataxia. • The presentation of MJD/SCA3 varies greatly but always includes ataxia. This affected mother and daughter both suffer from mild, progressive gait ataxia accompanied by mild scanning dysarthria, mild incoordination, and, in the mother’s case, ophthalmoparesis noted on lateral gaze. They represent an unusual pair of cases because their disease repeat lengths were classified by the gene testing service as “intermediate size alleles of indeterminate significance.” Their repeats (54 and 52, respectively) were slightly smaller than the accepted repeat range of >56; in contrast, normal repeats are 42 or smaller for this gene. The ataxic presentation in this mother-daughter pair illustrates that “intermediate” repeat lengths can in fact cause disease. When interpreting the significance of repeat lengths in dynamic repeat diseases, the clinician should use clinical judgment to help determine whether those uncommon repeat lengths falling within a “gray” area are actually the cause of disease.
References • Blumenfeld • Brazis Thanks