Download
1 / 1
80 likes | 327 Views
Background. Key Steps continued. Key Steps continued. Key Steps continued. Step 3 Evaluation. Step 2 Implementation of Med Rec (Pilot in Medical Floor). Step 2 Implementation of Med Rec. Step 1 Development of Process Develop Team/FMEA

E N D
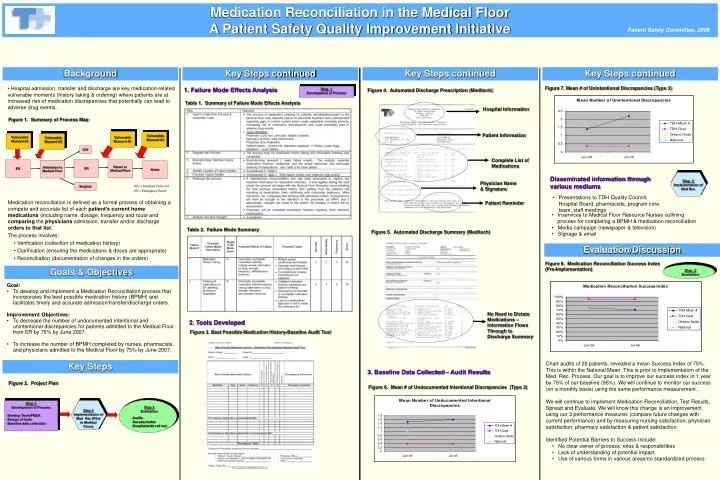
Background Key Steps continued Key Steps continued Key Steps continued Step 3 Evaluation Step 2 Implementation of Med Rec (Pilot in Medical Floor) Step 2 Implementation of Med Rec • Step 1 • Development of Process • Develop Team/FMEA • Design of tools • Baseline data collection Step 3 Evaluation • Audits • Success Index • Hospital-wide roll out Medication Reconciliation in the Medical Floor A Patient Safety Quality Improvement Initiative Patient Safety Committee, 2006 • Hospital admission, transfer and discharge are key medication-related vulnerable moments (history taking & ordering) where patients are at increased risk of medication discrepancies that potentially can lead to adverse drug events. Figure 7. Mean # of Unintentional Discrepancies (Type 3) 1. Failure Mode Effects Analysis Step 1 Development of Process Figure 4. Automated Discharge Prescription (Meditech) Table 1. Summary of Failure Mode Effects Analysis Hospital Information Figure 1. Summary of Process Map Vulnerable Moment #3 Patient Information Vulnerable Moment #4 Vulnerable Moment #1 Vulnerable Moment #2 ICU Complete List of Medications OR ER Return to Medical Floor Admission to Medical Floor Home Disseminated information through various mediums Physician Name & Signature Surgical ICU = Intensive Care Unit ER = Emergency Room • Presentations to TDH Quality Council, • Hospital Board, pharmacists, program core • team, staff meetings • Medication reconciliation is defined as a formal process of obtaining a compete and accurate list of each patient’s current home medications (including name, dosage, frequency and route and comparing the physicians admission, transfer and/or discharge orders to that list. • The process involves: • Verification (collection of medication history) • Clarification (ensuring the medications & doses are appropriate) • Reconciliation (documentation of changes in the orders) Patient Reminder • Inservices to Medical Floor Resource Nurses outlining • process for completing a BPMH & medication reconciliation • Media campaign (newspaper & television) • Signage & email Table 2. Failure Mode Summary Figure 5. Automated Discharge Summary (Meditech) Evaluation/Discussion Figure 8. Medication Reconciliation Success Index (Pre-Implementation) Goals & Objectives • Goal: • To develop and implement a Medication Reconciliation process that incorporates the best possible medication history (BPMH) and facilitates timely and accurate admission/transfer/discharge orders. • Improvement Objectives: • To decrease the number of undocumented intentional and unintentional discrepancies for patients admitted to the Medical Floor from ER by 75% by June 2007. • To increase the number of BPMH completed by nurses, pharmacists, and physicians admitted to the Medical Floor by 75% by June 2007. No Need to Dictate Medications – Information Flows Through to Discharge Summary 2. Tools Developed Figure 3. Best Possible Medication History-Baseline Audit Tool • Chart audits of 20 patients, revealed a mean Success Index of 75%. This is within the National Mean. This is prior to implementation of the Med. Rec. Process. Our goal is to improve our success index in 1 year by 75% of our baseline (95%). We will continue to monitor our success (on a monthly basis) using the same performance measurement. • We will continue to implement Medication Reconciliation, Test Results, Spread and Evaluate. We will know this change is an improvement using our 3 performance measures (compare future changes with current performance) and by measuring nursing satisfaction, physician satisfaction, pharmacy satisfaction & patient satisfaction. • Identified Potential Barriers to Success Include: • • No clear owner of process, roles & responsibilities • Lack of understanding of potential impact • • Use of various forms in various areas/no standardized process Key Steps 3. Baseline Data Collected – Audit Results Figure 2. Project Plan Figure 6. Mean # of Undocumented Intentional Discrepancies (Type 2)