Download
1 / 38
410 likes | 804 Views
ENDOCRINE DISEASES. BY CYNTHIA L. DIETRICH, D.O. November 23, 2004. www.anaesthesia.co.in anaesthesia.co.in@gmail.com. DIABETES MELLITUS . Problem in glucose metabolism, accompanied by predictable long-term vascular and neurologic complications Chronic disease

E N D
ENDOCRINE DISEASES BY CYNTHIA L. DIETRICH, D.O. November 23, 2004 www.anaesthesia.co.inanaesthesia.co.in@gmail.com
DIABETES MELLITUS • Problem in glucose metabolism, accompanied by predictable long-term vascular and neurologic complications • Chronic disease • Significant morbidity and mortality
COMPLICATIONS • Hyperglycemia +/- ketoacidosis • Hypoglycemia: activation of the sympathetic nervous system (diaphoresis, tremulousness and tachycardia) and insufficient delivery of oxygen to the brain (confusion, seizures and unconsciousness
Retinopathy- microaneurysms cluster at macula->terminal vessels obstructed->ischemia->new vessel proliferation • Nephropathy-leads to hypertension. Assoc with the highest mortality. • Cardiovascular disease- “silent ischemia” • Peripheral neuropathy- numbness and tingling progressing to total insensitivity • Stiff joint syndrome- “prayer sign” and atlanto-occipital joint involvement
Autonomic nervous system dysfunction -orthostatic hypotension, resting tachycardia, absent beat-to-beat variation -hypogylcemic unawareness -gastroparesis occurs in 20-30%
IDDM • Prevalence 0.4% • Onset most often prior to age 20 • Environmental influences are superimposed on a genetic component located on chromosome 6 • Absolute insulin deficiency • Pancreatic beta islet cells are destroyed and anti-islet cell antibodies appear • Clinical symptoms when 90% of the beta cells destroyed • Associated with other autoimmune diseases: rhuematoid arthritis and thyroid disease
Clinical presentation is unmistakable: hypergylcemia, polyuria, polydipsia, weight loss, blurred vision and ketoacidosis • Long term management requires exogenous insulin, self monitoring, lifestyle adaptations including diet and exercise • Insulin formulations rapid (regular), intermediate (Lente, NPH) or long-acting (Ultralente) • Goal- HbA1c less than 7.5%
DKA • Insulin transfers glucose and amino acids into the cells. • Hyperglycemia->osmotic diuresis->dehydration->acidosis. Also, a build up of amino acids in the blood->lipolysis->free fatty acids->converted to ketone bodies in the liver • Results in a intravascular fluid volume deficit of 5-8 liters, potassium deficit of 200-400 mEq, and NaCl deficit of 350-600 mEq
Treatment of DKA • Intubate for CNS depression • Regular insulin 10 units IVP followed by 5-10 units/hr IV • Normal saline 5-10 ml/kg/hr IV • Add 5% glucose when serum blood sugar<250 mg/dl • Potassium 0.3-0.5 mEq/kg/hr IV • Monitor blood sugar, potassium, arterial pH and urine ketones hourly • Identify cause (sepsis, MI, compliance)
ANESTHETIC MANAGEMENT • Goal- blood sugar between 120-180 mg/dl • Surgery scheduled early in the day • ¼ to ½ usual daily dose of intermediate acting insulin on the morning of surgery • Frequent blood sugar analysis, q 1-2 hours intraop • Treat blood sugar values above 250 mg/dl
Tracheal intubation in patients with autonomic nervous system neuropathy (pre-treat with metoclopramide) • Choice of drugs for induction and maintenance less important than monitoring of serum blood sugar • +/- regional anesthesia due to peripheral neuropathies • Risk of peripheral nerve injury with positioning • Bradycardia and hypotension may require epi
NIDDM • Obese, sedentary lifestyle, and advancing age • Prevalence 6.6% • Insulin resistance and a decrease in insulin secretion • Usual onset after age 40 • Insulin resistance is inherited • Ketosis-resistant
Insulin-mediated stimulation of tyrosine kinase is impaired. This is necessary for normal function of insulin receptors. • Effect is reversible with improved control of serum blood sugar • When dietary management fails hypoglcemic drugs stimulate endogenenous insulin secretion, or inhibit gluconeogenesis in the liver and kidneys, and increase glucose uptake in skeletal muscles • Duration can be up to 36 hours
HYPEROSMOLAR, HYPERGLYCEMIC NONKETOTIC COMA -elderly, insulin deficiency, renal insufficiency, thirst deficiency -sepsis, hyperalimentation or drugs (corticosteriods) -glucose >600 mg/dl -osmotic diuresis->hypokalemia and dehydration -serum osmolarity >350 mOsm/L -pH >7.3 -hypovolemia (severe, up to 25% total body water) -patients are insulin deficient but liver insulin levels sufficient for metabolism of free fatty acids->no ketosis -coma due to shrinkage of brain cells
TREATMENT OF HHNC • Regular insulin 10 units IVP then recheck • Isotonic salt solution 2-3 liters over the first 1-2 hours • Subsequent half-strength saline • When plasma glucose level approaches normal start D5W • When urine output is resumed supplement potassium • Remember: this can be reversed with fluids alone, go slowly
ANESTHETIC MANAGEMENT • Same as IDDM except omit oral hypoglycemic the morning of surgery • Keep in mind long duration of action of oral hypoglycemic drugs • Obesity considerations
GESTATIONAL DIABETES • Glucose intolerance first detected during pregnancy • 2-3% of all pregnancies • Detected in the last trimester • Resembles NIDDM (50% develop NIDDM within 10 years) • Risk factor for fetal morbidity • Neonatal hypoglycemia • Increased Respiratory Distress Syndrome, cardiomegaly and congenital abnormalities
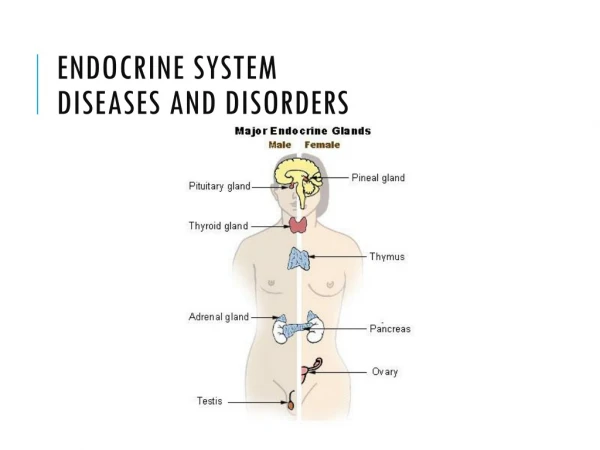
THYROID GLAND DYSFUNCTION • Overproduction or underproduction of T3 and/or T4 • Negative feedback regulated by the anterior pituitary gland and the hypothalmus • T3 and T4 act on cells through the adenylate cyclase system, producing changes in speed of biochemical reactions, total body oxygen consumption, and heat production
HYPERTHYROIDISM • Prevalence: 2% women, 0.2% men • Decreased TSH and increased T4 • Causes: Grave’s Disease, iatrogenic, Toxic nodular goiter and Thyroiditis • Signs and symptoms: goiter, tachycardia, anxiety, tremor, heat intolerance, fatigue, weight loss, eye signs, skeletal muscle weakness and atrial fibrillation • Stimulation of the sympathetic nervous system
TREATMENT OF HYPERTHYROIDISM • Antithyroid drugs: (methimazole, carbimazole, propylthiouracil) inhibit oxidation/formation of iodothyromines before treatment with radioiodine or surgery • B-adrenergic antagonists (propranolol, nadolol, atenolol) decrease some of the tachycardia, anxiety and tremor • Inorganic iodine inhibits the release of T4 and T3 for a limited time to prepare pt’s for surgery or treat thyrotoxic crisis
Radioiodine therapy destroys thyroid tissue • Subtotal thyroidectomy when radioiodine is refused or a large goiter is present causing tracheal compression or cosmetic concerns
ANESTHETIC MANAGEMENT OF HYPERTHYROIDISM • Elective surgery should be deferred until the patient is rendered euthyroid and hyperdynamic state controlled with B-blockers • Preop: anxiolytics and evaluation of upper airway (CT scan of the neck) • Induction: Thiopental has antithyroid activity (no ketamine) • Maintenance: isoflurane or sevoflurane (no halothane) and fentanyl or remi. Attention to body temp, heart rate and eye protection (exothalmos) • Muscle relaxation: avoid pancuronium and use glycopyrrolate with reversal agent • Treat hypotension with phenylephrine
COMPLICATIONS OF SUBTOTAL THYROIDECTOMY • Damage to the recurrent laryngeal nerve when unilateral->hoarseness, when bilateral->total airway obstruction • Damage to superior laryngeal nerve can lead to aspiration • Airway obstruction from tracheomalacia (after extubation) or hematoma (early postop period) • Hypoparathyroidism-> hypocalcemia develops 24-72 hours postop (but sometimes 1-3 hours postop)->laryngeal stridor->laryngospasm
THYROTOXIC CRISIS (THYROID STORM) • Medical emergency • Typically presents 6-18 hours after surgery • Abrupt onset of tachycardia, hyperthermia, agitation, skeletal muscle weakness, congestive heart failure, dehydration and shock due to abrupt release of T4 and T3 into the circulation • Precipitated by surgery, infection, trauma, toxemia, DKA
TREATMENT OF THYROID STORM • Intraveneous cooled crystalloid solutions, acetominophen and cooling blankets • Esmolol infusion with goal heart rate <100 • Potassium iodide to block release of T4 and T3 • Propylthiouracil 100 mg po to inhibit conversion of T4 to T3 • Cortisol 100-200 mg IV
HYPOTHYROIDISM • Prevalence 0.5-0.8% • Increased TSH and decreased T4 and T3 • Cause is primarily treatment of hyperthyroidism, medically or surgically or Hashimoto’s Thyroiditis • Signs and symptoms: lethargy, hypotension, bradycardia, CHF, gastroparesis, hypothermia, hypoventilation, hyponatremia, and poor mentation • Treatment with Synthroid
ANESTHETIC MANAGEMENT OF HYPOTHYROISM • Preop meds titrate and consider supplemental cortisol • Induction: ketamine • Maintenance: nitrous oxide plus short acting opioids, benzo’s or ketamine • Low dose muscle relaxants • Controlled ventilation of the lungs (vulnerable to excessive decrease in PaCO2) • Treat hypotension with ephedrine • Watch for CHF, consider arterial line and PA catheter
ADRENAL GLAND DYSFUNCTION • Hypercortisolism= Cushing’s Syndrome • Hypocortisolism= Addison’s Disease • Pheochromocytoma
CUSHING’S SYNDROME • Caused by excessive secretion of corticotropin by anterior pituitary corticotroph tumors (microadenomas) • Increased aldosterone, cortisol and testosterone in the adrenal cortex • Signs and symptoms: hypertension, hypokalemic alkalosis, hyperglycemia, hypernatremia, osteoporosis, easy bruising, polyuria, buffalo hump, moon facies, excessive body hair, menstrual abnormalities, weight gain, skeletal muscle wasting/weakness, depression and insomnia
Diagnosis with 24 hour urinary secretion of cortisol • Dexamethasone suppression test distinguishes Cushing’s disease from the ectopic corticotropin syndrome • Treatment of choice is transsphenoidal microadenomectomy or 85-90% resection of the anterior pituitary gland
ANESTHETIC MANAGEMENT • Preop evaluation of systemic blood pressure, electrolyte balance and the blood glucose • No single anesthetic the best • Replacement therapy hydrocortisone 10 mg/ hr for 24 hours • Treat hypertension and hypervolemia with a potassium sparing diuretic • Treat hyperglycemia with insulin • Care when positioning patient due to osteoporosis
CORTISOL • THE ONLY ESSENTIAL HORMONE FOR LIFE • Maintains blood pressure by facilitating the conversion of norepi to epi • Converts amino acids to glucose • Suppresses inflammation
ADDISON’S DISEASE • Absense of cortisol and aldosterone due to destruction of the adrenal cortex • Causes: hemorrhage in anticoagulated patients, sepsis, surgical or accidental trauma • Diagnosis by measurement of plasma cortisol before and 1 hour after administration of corticotropin • Signs and symptoms: weight loss, skeletal muscle weakness, hypotension, fluid depletion, hyperkalemia, hyponatremia, hypoglycemia, abdominal/back pain
MANAGEMENT OF A PATIENT WITH ADDISON’S DISEASE • You must give exogenous corticosteriods! • Intraveneous infusion of sodium containing fluids • Invasive monitoring with arterial line and CVP or PA catheter • Frequent measurements of glucose and electrolytes • Decrease initial dose of muscle relaxants
PHEOCHROMOCYTOMA • Catecholamine-secreting tumor that originates in the adrenal medulla or in the chromaffin tissues along the paravertebral sympathetic chain, extending from the pelvis to the base of the skull • Age: 30-50 years • 50% deaths occur during unrelated surgery or pregnancy • Diagnosis by 24 hour urine for norepinepherine and CT scan • Associated with Multiple endocrine neoplasia (MEN)
Signs and symptoms: tachycardia, diaphoresis, headache, hypertension, hyperglycemia, hypovolemia, tremulous, palpitations, weight loss • Treatment is surgical excision of the tumor(s)
ANESTHETIC MANAGEMENT OF PHEOCHROMOCYTOMA • Correct hypovolemia (serial hematocrits) • Alpha blockade before beta blockade • Alpha blockage: phenoxybenzamine 10-20 mg PO bid for 14 days pre-op • Beta blockade: propranolol 40 mg PO bid pre-op • Pre-op: benzo with scopalamine • Avoid histamine releasing drugs • Arterial line pre-induction
Induction: etomidate, thiopental or propofol • Lidocaine 1-2 mg/kg prior to intubation • Consider PA catheter • Maintenance: sevoflurane due to rapid changes in concentration and fentanyl or remifentanyl • Treat hypertension with phentolamine 1-5 mg IV or nitroprusside • Treat reflex tachycardia with an esmolol infusion www.anaesthesia.co.inanaesthesia.co.in@gmail.com