Download
1 / 49
520 likes | 537 Views
Mr. Samir Rahmani Consultant Upper GI and General Surgeon Nevill Hall Hospital. Obesity, Cancer and Endocrine. Body Mass Index (BMI). Under 18.5 is underweight 18.5 - 25 is healthy weight 25 - 30 is overweight 30 - 40 is obese Over 40 is morbid obese

E N D
Mr. Samir Rahmani Consultant Upper GI and General Surgeon Nevill Hall Hospital Obesity, Cancer and Endocrine
Body Mass Index (BMI) • Under 18.5 is underweight • 18.5 - 25 is healthy weight • 25 - 30 is overweight • 30 - 40 is obese • Over 40 is morbid obese * Obesity increase the risk coronary artery disease, diabetes mellitus, strokes, hypertension, sleep apnea, respiratory problems and osteoarthritis, social, work Related problems.
Obesity in the UK Health survey for England (HSE) data (Jan 2016) • 60% of adults are overweight or obese • 24% men and 27% women • Common to be overweight than obese • 1 in 10 children between 2-10 years, are obese • £4 billion per year spent on obesity related illnesses • Obesity reduces life expectancy by an average 9y
The World Health Organisation (WHO) 2015 Overweight and Obesity • GP records of more than 5 million people and the 22 cancer sites. • 10 different types of cancer (after tobacco). • Overweight and obesity lead to 18,000 cancer/year. • Prediction: 3/4 adults will be overweight or obese by 2035. • Extra 670,000 cancer in the UK over the next twenty years.
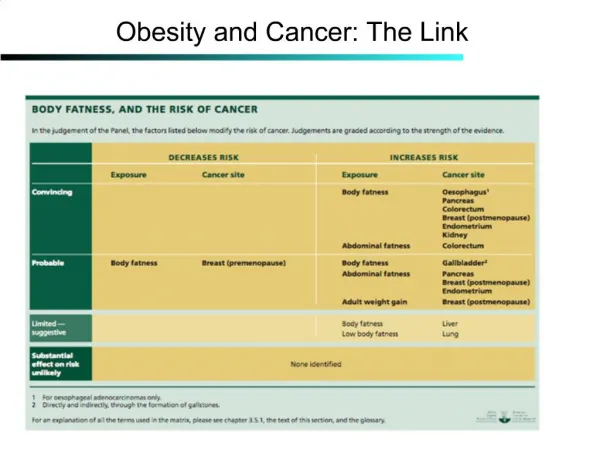
Obesity and Cancer • Definite link: Breast cancer Colon cancer Endometrial cancer • Strong link: Oesophageal Gastric Renal ca • Possible link: Prostate ca Gallbladder Pancreas Ovary Lymphoma Multiple myeloma Obesity increase risk of recurrence
Polednak AP et al (2003) • US study • 25 years of cancer registry data from different parts of the US • Increasing cancers in the obese population • Nearly 40,000 cancers diagnosed in 2002 linked to obesity
Catalán V et al (Sep 2016) USA • 34,000 new cases of cancer in men and 50,500 in women were due to obesity, particularly endometrial cancer and oesophageal Ca. • Obese patients with CC exhibit increased levels of circulating ECM proteins (OPN, YKL-40 and TNC) which an be used as a Dx biomarkers. • in 2030, about 500,000 additional cases of cancer • BMI reduction by 1%, will avoid 100,000 new cases of cancer by 2030
Calle EE et al 2003 • Prospective study of 900,000 people over 16 years • 52% ↑ cancer related mortality in obese men • 62% ↑ cancer related mortality in obese women • 15-20% cancer deaths related to obesity
Pathophysiology of Cancer in Obese • High Oestrogen level (Breast, Endometrial). • ↑ Insulin & resistance, (Oesophageal, Gastric, Colon). • High adipokines level, which has a proliferative effects (Renal, Colon) • Modulating immune responses • Chronic low grade inflammatory state in the fatty tissues • Sex hormones bioavailability • Effects on kappa beta system • Oxidative stress
Obesity and Breast cancer • Mainly in post-menopausal women • Lahmann et al (2003): 12,000 post-menopausal women 6 years follow up ↑ BMI, ↑ percent body fat, fat distribution • Increased mortality from breast Ca
Obesity and Endometrial cancer • Up to 4 times increased risk in obese women • May account for 40% of endometrial ca in the Western world • Dossus et al (2010) 300 endometrial Ca vs 570 controls Obesity with elevated CRP, IL6 and IL1Ra increases risk X 4 times of Endo Ca.
Obesity and CRC • Increased risk in obese and overweight population • American Cancer Society study: • Nearly a million people studied over 12 years • Increased cancer mortality in obese men • Weaker association in obese women
Oesophageal / Gastric Ca • Progressive rise in incidence • Possible link with GORD in obese people • Whiteman et al (2008): • 800 cases of oesophageal / cardia tumours • Obesity + reflux combination significantly increases risk • Lesser association in women
Anti-obesity Surgery • Achieves dramatic weight loss • Reduce the risk of cancer • Hypertension • Diabetes • Sleep apnea & COPD • OA • Social
Does Bariatric surgery reduce cancer risk ? • Swedish Obese Subjects Study • Prospective study of 4000 obese patients • 2000 underwent bariatric surgery • Patients followed up between 1987 – 2005 • Significant reduction in cancer incidence in women • No difference in men
Bariatric surgery and Cancer risk • Christou et al (2008) • 1000 bariatric surgery patients vs 5000 controls • Reduced cancer risk in surgery group, especially breast Ca
Ted D. Adams et al 2015 • Reduced cancer mortality following bariatric surgery • Cancer mortality was 46% lower in the surgery group compared to controls • Significant reduction in total cancer mortality in gastric bypass patients compared with other modes of surgery.
CHARLOTTESVILLE, Va. et al Oct 2015 Bariatric surgery on obese women eliminates precancerous uterine growths Alba Maestro et al August 2014Bariatric surgery has a protective effect from overall cancer risk, mainly in women
Reducing cancer risk without surgery • Avoiding weight gain • Increased physical activity • Experimental drugs such as Metformin, Statins, Thyroxine
Ideal Bariatric Procedure • Achieves 70-100% excess weight loss. • Causes maintained weight loss. • Simple with low operative risks. • Minimal side effects. • Maintain absorption of trace elements
Calculating Excess weight loss • BMI= wt/ht2(m) • wt=120kg Ht= 1.6m BMI=46.8 • Ideal BMI (25) X (1.6)2 =64kg (ideal wt) • Excess wt= current wt - ideal wt • Excess wt= 120 – 64= 56kg • 70% to 100% EWL= 39kg to 56kg
Current Bariatric Procedures • Gastric banding • Sleeve Gastrectomy • Gastric bypass • Duodenal switch • Biliopancreatic diversion • Vertical banding gastroplasty
Gastric Band (AGBP) • Easy • Cheap • Achieve wt loss • Perforation • Dysphagia • Migration • Failure
Sleeve Gastrectomy (SG) • Relatively simple • Achieve reasonable weight loss • 32Ch gastric bougie • Staples 5cm proximal to pylorus • Useful for BMI 25-40 • Not maintained weight loss
Gastric Bypass (RYGB) • Relatively simple • Achieves good weight loss • Maintained weight loss • No access to remaining stomach • No access to biliary system • Dumping • Denied duodenal absorption
Duodenal Switch (DS) • More demanding • Very good weight loss • Maintained weight loss • No dumping • No access to biliary system • Denied duodenal absorption
Vertical banding gastroplasty Biliopancreatic diversion Both are abandoned
Laparoscopic Sleeve Gastrectomy (LSG) • Achievement of good/maintained weight loss • Access to biliary system • Maintained duodenal abdsorption • Restrictive and Malabsorptive
Technique • LSG • Stapling at 5cm away from the pylorus
Patients Demographs • 255 patients had LSG • Age: 19 – 65 years (mean 47 years) • Weight: 98 -194 Kg (mean 144 Kg) • BMI: 39 – 67 (mean BMI 52)
Follow up • F/U at 3/6/12 months, then annually. • January 2004 January 2017 = 323 pts. • 260 patients are followed up 2 years.
Follow up Clinical Biochemical Weight and BMI Eating habits Diabetes and Blood pressure Bowel habits Signs of vitamin deficiency Full blood count Liver function tests Urea and electrolytes Trace elements (Zinc, copper, selenium) Vitamins A, B6, B12, D, E
Results • % EWL 64 – 104% (Mean 77%) • BMI 24 – 34 (Mean 29.5) • Trace elements deficiency in 24.6 % (Zinc & Selenium) • Vitamin D and/or B12 deficiency in 29.2 % • 5% less chance of malnutrition • Less N+V compared to other procedures
Results • 85% resolution of diabetes mellitus II • 43% resolution of diabetes mellitus I • 90% cure of high blood pressure • No change in bowel habits in any of the patients • Normal liver enzymes in all patients
Long term follow up • Maintenance of previous weight +/- 3 Kg • Trace elements deficiency corrected by oral supplementation • Vitamin deficiency corrected by oral tablets • Excellent eating satisfaction
Conclusion • LSG is an excellent Bariatric operation • Achieves good and maintained weight loss • No dumping • Access to remaining stomach/biliary system • Minimal side effects and nutrients absorption in the duodenum • One-stage simple operation for patients with high BMI
Obes Surg. 2016 Oct;26(10):2316-23. doi: 10.1007/s11695-016-2098Medium-Term Results of Combined Laparoscopic Sleeve Gastrectomy and Modified Jejuno-Ileal Bypass in Bariatric Surgery.Hassn A, Luhmann A, Rahmani S, Morris-Stiff G
Open Access Maced J Med Sci. 2017 Jun 11;5(3):316-318. doi: 10.3889/oamjms.2017.074. The Role of Sleeve Gastrectomy on Preventing Type 2 Diabetes Mellitus. Özdaş S1, Olt S2, Şirik M3. In this present study we found that bariatric surgery caused a significant decrease in HbA1c levels in non-diabetic patients, suggesting that bariatric surgery may prevent Type 2 Diabetes Mellitus in obese patients.
Am J Physiol Endocrinol Metab. 2017 Jul 11:ajpendo.00042.2017. doi: 10.1152/ajpendo.00042.2017. Glycemic control after metabolic surgery: a Granger causality and graph analysis. 85% resolution Previti E1, Salinari S1, Bertuzzi A2, Capristo E3, Bornstein S4, Mingrone G5.
A prospective 4-year study of insulin resistance and adipokines in morbidly obese diabetic and non-diabetic patients after gastric banding. Urbanavicius V1, Juodeikis Z2, Dzenkeviciute V1, Galkine A1, Petrulioniene Z3, Sapoka V1, Brimiene V2, Vitkus D4, Brimas G2. The most significant metabolic changes occurred within 1 year after LAGB. The 4-year follow-up revealed stabilization in metabolic indices rather than significant improvement.
Long-term outcome of laparoscopic sleeve gastrectomy from a single center in mainland China. Hans PK1, Guan W1, Lin S1, Liang H2. CONCLUSION: LSG is a safe and effective procedure with good five year results. Weight regain remains a concern two years post surgery. S
Angiology. 2017 Jan 1:3319717718707 Sleeve Gastrectomy Efficacy on Metabolic and Cardiovascular Dysfunction With a Focus on the Role of Comorbidities. Ricci MA1, Ministrini S1, De Vuono S1, Camilli M1, Gentili A1, Daviddi G1, Boni M2, Lupattelli G1. Diabetic patients experienced a greater improvement in systolic blood pressure, and high-density lipoprotein cholesterol than nondiabetics. Patients with diabetes and hypertension experienced a greater improvement in vascular and metabolic status after SG.
Curr Diab Rep. 2017 Aug;17(8):62. doi: 10.1007/s11892-017-0887-y. Bariatric Surgery for Adolescents with Type 2 Diabetes: an Emerging Therapeutic Strategy. Stefater MA1, Inge TH2. Paralleling what has been seen in adult patients, bariatric surgery dramatically improves glycemic control in patients with T2D. In fact, remission of T2D has been observed in as many as 95-100% of adolescents with diabetes after bariatric surgery, particularly vertical sleeve gastrectomy (VSG) and Roux-en-Y gastric bypass (RYGB) surgery. Bariatric surgery including RYGB and VSG is a powerful therapeutic option for obese adolescents with T2D. Benefits must be weighed against risk for postoperative complications such as nutritional deficiencies, but earlier surgical intervention might lead to more complete metabolic remission in obese patients with T2D.
Obes Surg. 2017 Jun 26. doi: 10.1007/s11695-017-2777-4. [Epub ahead of print] Laparoscopic Sleeve Gastrectomy for the Management of Type 1 Diabetes Mellitus. Al Sabah S1, Al Haddad E2, Muzaffar TH2, Almulla A2. The prevalence of obesity is on a continuous rise worldwide, with major studies clearly correlating obesity with the development of chronic metabolic disorders including type 2 diabetes. Bariatric surgery has proven to be beneficial in the management of this condition; however, a limited number of studies exist on its effect on type 1 diabetes. Laparoscopic sleeve gastrectomy resulted in significant weight loss, comorbidity resolution as well as reduction in their insulin doses post-op. However, glycemic control does not seem to show significant improvement in these patients. Larger, more long-term studies are needed to reach a definite conclusion on this topic.