Download
1 / 62
620 likes | 721 Views
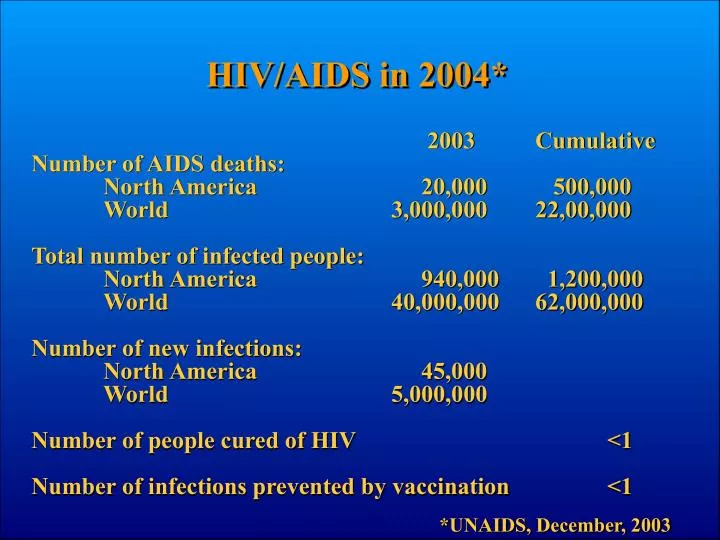
HIV/AIDS in 2004*. 2003 Cumulative Number of AIDS deaths: North America 20,000 500,000 World 3,000,000 22,00,000 Total number of infected people: North America 940,000 1,200,000 World 40,000,000 62,000,000 Number of new infections:

E N D
HIV/AIDS in 2004* 2003 Cumulative Number of AIDS deaths: North America 20,000 500,000 World 3,000,000 22,00,000 Total number of infected people: North America 940,000 1,200,000 World 40,000,000 62,000,000 Number of new infections: North America 45,000 World 5,000,000 Number of people cured of HIV <1 Number of infections prevented by vaccination <1 *UNAIDS, December, 2003
The HIV Replication Cycle Entry via fusion Following coreceptor binding Adsorption to CD4 receptor Nef Reverse transcription Gag-Pro-Pol Integration splicing Assembly Budding Tat Vif Maturation Rev Vpu Transcription
Important Properties of HIV • Infection requires CD4 protein on the surface of the cell as receptor. • Therefore can only infect CD4+ (“helper”) T cells and a few others. • Almost all infected cells die within a day or two after infection. • Infected CD4 cells make enough virus particles to infect about the same number of new cells (10-100 million). • Therefore, the infection in an individual persists by constant, repeated cycles of infection and cell death (about 1 a day). • These properties are also found in the benign SIV-monkey infections, but in humans there is a slow loss of total CD4 cells, leading eventually to failure of the immune system.
+ (copies/ ml plasma) HIV RNA l ) CD4 T cells (cells/ m
Appearance of 3TC-Resistant Mutations in Treated Patients RNA Copies/ml
5 10 10 4 10 10 3 10 10 "Undetectable" 2 10 10 b e r o f i n f e c t e d c e l l s A p p r o x i m a t e n u m 1 10 10 0 10 10 -1 10 10 -1 10 10 "Eradication" -3 10 10 2 3 0 1 8 7 6 5 Virus load (copies/ml) 4 3 2 1 0 Years
Persistence of Cells latently Infected with HIV after Suppression of Viremia to “Undetectable” Levels Zhang et al NEJM 340:1605-1613
Viremia Persists after Suppression by Antiretroviral Therapy 107 Start Therapy (D4T/3TC/efavirenz) 106 Start Therapy (D4T/3TC/efavirenz) 105 104 103 102 101 4 ± 2 c/ml 22 ± 6 c/ml 100 10-1 bDNA bDNA <75 copies/ml Single Copy Assay Single Copy Assay < 1 copy/ml 107 106 105 104 Plasma HIV-1 RNA (copies/ml) 103 102 101 100 10-1 0 200 400 600 800 0 200 400 600 800 Time (days) Time (days)
HIV-Host Interaction 1. After early primary infection, HIV gives lifelong persistent infection leading to AIDS after about 10 years (on average). 2. Persistence is due to constant replication of the virus and killing of 107-109 infected CD4+ T cells at about 1 cycle/day. 3. Smaller fractions of “latently infected” cells that live much longer after infection are probably unimportant for the natural history of the infection, but very important for foiling treatment. 4. Constant replication day after day, year after year, leads to extensive genetic variation. • Antigenic escape. • Drug resistance. • Variation in coreceptor usage. 5. The system remains in an extraordinarily robust quasi steady state for thousands of replication cycles before progressing to disease. 6. We still don’t know how HIV causes AIDS.
HIV Drug Resistance • Introduction. • Mechanism of resistance. • Evolution of resistance.
The HIV Replication Cycle Entry via fusion Following coreceptor binding Adsorption to CD4 receptor Nef Reverse transcription Gag-Pro-Pol Integration splicing Assembly Budding Tat Vif Maturation Rev Vpu Transcription
Anti-HIV Therapies Unsuccessful (so far): • Immunotherapy. • Gene therapy. • Recombinant antiviral proteins. • Herbal extracts. • Faith healing. Successful: • Nucleoside RT inhibitors. (AZT, 3TC, ddI, ddC, d4T, etc.) • Non nucleoside RT inhibitors. (Nevirapine, Efavirenz, Delavirdine,etc.) • Protease inhibitors. (Indinavir, Saquinavir, Nelfinavir, Ritonavir, etc.) • Fusion inhibitors (Enfuvirtide). Promising: • Integrase inhibitors. • Coreceptor inhibitors.
Approved anti-HIV Drugs2003 • Protease Inhibitors: • Nucleoside RT • Inhibitors: • Nonnucleoside RT Inhibitors: • Fusion Inhibitors: • Abacavir • Amprenavir • Enfuvirtide • (T20) • Delavirdine • Didanosine (ddI) • Indinavir • Efavirenz • Lamivudine (3TC) • Lopinavir • Nevirapine • Nelfinavir • Ritonavir • Saquinavir • Stavudine (d4T) • Tenofovir • Zalcitabine (ddC) • Zidovudine (AZT)
p r o t e a s e i n h i b i t o r T h e r a p y w i t h a t i e n t - d a y s % o f p a Deaths per 100 person-years
HIV Drug Resistance 1. Occurs with all (effective) antivirals tested to date, in vivo and in vitro. (“If you don’t get resistance, the drug’s no good.”) 2. Is the most important factor preventing successful long term treatment. (If resistance did not arise, we would probably not be here today.) 3. Monotherapy almost always rapidly fails, most likely due to selection of mutants already present in the virus population. 4. Our only way to deal with this problem at present is to throw enough drugs at it so that no preexisting variant is resistant to all of them, and that replication is sufficiently suppressed to prevent further evolution. 5. A patient for whom this therapy has failed has very few treatment options left.
Location of Drug Resistant Mutations in HIV Proteins A. Reverse transcriptase Nucleoside RT inhibitors Nonnucleoside RT inhibitors Pyrophosphate RT inhibitors Protease inhibitors Fingers Palm Palm Thumb Connection RNase H Fingers Integrase inhibitors Binding/fusion inhibitors B. Protease C. Integrase D. Env gp120SU gp41TM V1 V2 C2 V3 C3 V4 C4 V5 Ectodomain Cytoplasmic domain C1 600 700 800 900 0 100 200 300 400 500 Amino Acid Position
Drug-Resistant Mutations in HIV • NNRTI’s • 3TC • AZT • Protease inhibitors
thumb RNase H p66 RNase H active site primer palm pol active site template p51 fingers Courtesy of E. Arnold
Locations of Drug Resistance Mutation Sites in HIV-1 RT/DNA Structure Nucleoside drug resistance mutation sites Non-nucleoside drug resistance mutation sites
NNRTI Resistance • Occurs rapidly in patients and cell culture. • Virtually complete cross-resistance to chemically very different compounds. • Mutations in binding “pocket” at base of thumb domain. • Pocket does not exist in the native structure.
Binding of NNRTIs to HIV-1 RT Courtesy of E. Arnold
NNRTI binding pocket region in wild-type HIV-1 RT structure Lys 102 Leu 100 Lys 101 Tyr 181 p51 OW Lys 103 Glu 138 (B) Tyr 188 b6 b10 b9 Courtesy of E. Arnold
Leu 234 Tyr 318 Pro 95 Trp 229 Leu 100 Phe 227 Pro 236 Lys 103 Tyr 181 Val 106 Tyr 188 Gly 190 Inhibitor-protein Interactions Interactions are predominantly hydrophobic (with side-chains of L100, Y181, Y188, F227, W229, L234, and Y318). Courtesy of E. Arnold
NNRTI binding pocket region in K103N/Y181C mutant structure Asn 136 (B) Lys 101 Leu 100 2.8 Å Lys 102 OW Glu 138 (B) 3.3 Å Asn 103 3.1 Å Cys 181 Tyr 188 b6 b10 b9 Courtesy of E. Arnold
3TC Resistance • Occurs rapidly in patients and cell culture. • Mutations nearly always at M184 in active site. • RT from resistant virus is resistant to 3TCTTP incorporation. • Resistance due to steric hindrance.
Structure of 3TC (-)-2´, 3´-dideoxy-3´-thiacytidine (3TC) Deoxycytidine 3TC
Steric Hindrance in 3TC Resistance 3TC dTTP Sarafianos, et al.,1999. PNAS USA 96: 10027-10032.
AZT Resistance • Occurs rapidly in patients and cell culture. • Mutations not at active site or dNTP binding site. • RT from resistant virus not resistant to AZTTP incorporation. • Resistance due to excision (pyrophosphorolysis).
Clash Between Incorporated AZT and Active site Aspartic Acid Prevents Translocation Courtesy of S. Hughes
Other NRTI AZT Courtesy of S. Hughes
Protease Inhibitor Resistance • Occurs rapidly in patients and cell culture. • Usually associated with multiple mutations that arise sequentially. • Initial (primary) mutations at or near active site, and often greatly reduce fitness. • Subsequent mutations often far away from active site (or even in gag), and, in many cases, act to improve fitness.
Evolution of Protease Inhibitor Resistance in Vivo Primary Secondary mutation mutations Relative virus load Time (weeks)
Modeling HIV Variation • How do drug resistance mutations arise?
Start 3TC Evolution of 3TC Resistance Virus Load Time, Weeks
Start 3TC Evolution of 3TC Resistance M184 (AUG) Virus Load M184V (AUG-GUG) M184I (AUG-AUA) Time, Weeks
Start 3TC Evolution of 3TC Resistance M184 (AUG) Virus Load M184V (AUG-GUG) M184I (AUG-AUA) Time, Weeks
Evolution of HIV in Infected People Thesis: 1. Drug-resistant mutations are present in the virus population prior to therapy. 2. In the absence of drug, these mutations are slightly deleterious to the virus.
Factors of HIV Evolution 1. Mutation
Factors of HIV Evolution 2. Selection More fit Less fit
Factors of HIV Evolution 3. Drift Mutant proportion changes due to random sampling More important in small populations of cells
Selection at linked sites is not independent, even in large populations. Deleterious mutations accumulate. Factors of HIV Evolution 4. Linkage Can be reversed by recombination or compensating mutations. Etc.
Accumulation of Drug Resistant Mutations Before Start of Therapy Large, Linkage Small Medium Large Population size: 1 / s 1 N s / m 0.03 . 0 3 0.02 Mutant frequency . 0 2 0.01 . 0 1 0 0 0 1000 2000 3000 (0) (5) (10) (15) Time, generations (years after infection)
Accumulation of Drug Resistant Mutations Before Start of Therapy Large, Linkage Plus recombination or compensating mutations Large, linkage Population size: 1 / s 1 N s / m 0.03 . 0 3 0.02 Mutant frequency . 0 2 0.01 . 0 1 0 0 0 1000 2000 3000 (0) (5) (10) (15) Time, generations (years after infection)
HIV Drug Resistance Program National Cancer Institute at Frederick Genetics of HIV-1 Populations in Infected Individuals
Objectives • To obtain a detailed analysis of HIV-1 genetic diversity in infected patients to understand: • Roles of mutation and selection. • Replicating population size. • Extent of recombination. • Presence of compensatory mutations.
Patients in Study • 1. Recent HIV infection (n=3) • 10-100 days post-infection • VL=12,000->500,000 copies/ml • 2. Chronic untreated HIV infection (n=3) • >4 mos-10 years • VL=7,300-30,000 copies/ml • 3. Chronic HIV infection initiating ART (n=3) • >6 mos-15 years • VL=86,000-1,500,000 copies/ml