Download

1 / 20
200 likes | 222 Views
This research evaluates the progression of Mild Cognitive Impairment to dementia using the Montreal Cognitive Assessment tool. Results suggest MoCA scores alone poorly predict advancement to dementia, highlighting the importance of considering age and cognitive impairment severity in MCI patients.

E N D
Severity of mild cognitive impairment does not predict progression!Dr. Howard Chertkow, Dr. Ziad Nasreddine, Dr. Natalie Phillips Dept. of Clinical Neuroscience and Div. of Geriatric Medicine, Jewish General Hospital, McGill University, Montreal, Canada
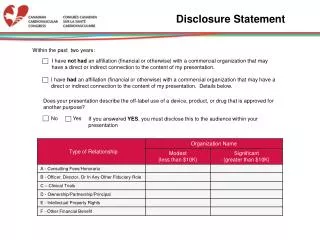
Disclosure Statement HC has been a paid consultant or received honoraria for participation in CME/advisory boards or grant funding from: Pfizer, Bristol-Meyers Squibb, Janssen-Ortho Inc., Lundbeck Canada
What is Mild Cognitive Impairment?(Petersen,Int. Psychogeriatr., 1997;9,45-55) • Subjective memory complaint • Preserved general intellectual function • Demonstration of objective memory impairment on cognitive testing • Intact activities of daily living • no other good explanation for memory loss • Not severe enough to meet criteria of dementia
Subjective Cognitive Impairment Objective Cognition MCI 100% 90% 15 years 7 years Alzheimer’s Disease 80% 70% 60% T minus 22 years T minus 7 years Time of Diagnosis B. Reisberg, IPA meeting, 2009
Natural History • 15% MCI per year initially progress to dementia • Even 10 years after initial onset of symptoms, 25% of cohort does not have dementia -their prognosis is not known • At present there is no simple way to predict who will progress and who will not
EarlyMCI LateMCI
MoCA Montreal Cognitive Assessment -a cognitive screening tool for detection of MCI Ziad S Nasreddine, Howard Chertkow, Natalie A Phillips J.Am Geriatr Soc 53:695–699, 2005 • One-page • 30-point scale • 10 minutes to administer • French/English • Tests 8 domains • Available at www.mocatest.org • Score<26 abnormal
Methods • 106 patients presenting in Memory Clinic at Jewish General Hospital (JGH) in Montreal 2005-2007 • All met clinical criteria for MCI [Petersen 2004] • Followed annually in clinic • Administered MoCA, neuropsych batteries. • Assessed clinically at each visit as ‘progressed to dementia’ (Progressors) vs ‘still MCI’ (Non-progressors) • Follow-up at least 1 year, usually 2 years
Distribution of Total initial MoCA scores in JGH MCI cohort (n=106) Over course of follow-up, 45 progressed to dementia (41/45=AD,rest mixed), and 61 did not progress to dementia.
JGH MCI Cohort 2005-07 t: Progressors and Non-progressors significantly different at p< 0.001 *: Progressors and Non-Progressors significantly different at p< 0.05
MoCA item analysis in Progressors vs. Non-Progressors (% pass where item is pass/fail; Avg +/- SD) *: Significant difference between progressors and non-progressors at p<0.05. **:Significant difference between progressors and non-progressors at p<0.01.
Distribution of P vs. NP in tertiles of MoCA total score Lowest tertile vs. Highest tertile: Continuity Corrected Chi Square=3.51, p=0.06
But… • When you control for the effect of age, the MoCA no longer distinguishes between P & NP (ANCOVA results: F(1,103)=2.2, n.s.).
Distribution of Progressors and Non-Progressors by age group Continuity Corrected Chi Square = 19.9, p.<0.001
Percentage of P vs. NP in 3 clinical strata of MoCA score Moderate deficit vs. mild or normal/minimal deficit (Combined): Continuity Corrected Chi Square=3.58, p=0.06
Scatterplot of MoCA scores by age with x & y axes meeting at cutoffs of MoCA=20 & age=75 (Progressors in red)
Breakdown of JGH Cohort by MoCA & Age cutoffs *: proportion of progressors in this group significantly different from proportion in Low MoCA older group and Higher MoCA older group as per Continuity Corrected Chi Square with p.<0.001 in both cases.
Conclusions • The MoCA score (and hence severity of cognitive impairment) alone, is a weak predictor of progression from MCI to dementia • Nevertheless, low MoCA scores (<20) along with age (≥75) define MCI patients at high risk of progression • Early MCI (minimal deficit) vs Mild MCI may not pick up different progression rates
Acknowledgements • Supported by the CIHR, Alzheimer’s Society of Canada, FRSQ (Quebec), and CDKTN (Canadian Dementia Knowledge Transfer Network).