Download
1 / 35
350 likes | 369 Views
This study explores the implications of VAD complications on transplant priority, analyzing mortality rates and categorizing subgroups based on INTERMACS definitions to inform prioritization decisions. The research aims to assess mortality risks post-complications and compare outcomes with non-MCS UNOS candidates using INTERMACS and OPTN data. The study investigates various complications including infections, device malfunction, bleeding, and arrhythmias among others to identify distinct risks within subgroups. The findings may influence transplant prioritization strategies.

E N D
Survival following VAD complications: implications for transplant priority. Todd Dardas, MD, MS May 16, 2015
Disclosures • Funding: • American College of Cardiology/Sankyo Daiichi Career Development Grant
Candidate survival Wever-Pinzon, O, et. al.; Circulation 2012
Status 1A exceptions Meyer D, et. al. American Journal of Transplantation 2015; 15: 44–54
UNOS 1A(b) justifications Unpublished data, UNOS registry
Tier Proposals • MCS with arrhythmias, non-dischargeable VAD • Device malfunction, IABP • MCS (infection, thromboembolism, other complications), LVAD 30 days, dual inotropes • Inotrope w/o HD monitor, stable VAD • Multi-organ transplants • Remaining candidates Meyer D, et. al. American Journal of Transplantation 2015; 15: 44–54
Guidance from OPTN • Aortic insufficiency • Hemolysis • Pump thrombosis • Pump-related local or systemic infection • Bleeding • Right heart failure • Recrudescent arrhythmias • Device malfunction Meyer D, et. al. American Journal of Transplantation 2015; 15: 44–54
OPTN infection guidance Pump-related or systemic infection with one of: • Symptoms along driveline with leukocytosis AND: + blood culture or + site culture • Surgical debridement of the driveline AND + site culture • + Pump pocket culture • Bacteremia with the same organism 4 weeks following treatment Meyer D, et. al. American Journal of Transplantation 2015; 15: 44–54; http://www.uab.edu/medicine/intermacs/appendices-4-0/appendix-a-4-0
Research aims • Determine mortality for complications following CF VAD placement and compare to non-MCS UNOS candidates. • Evaluate whether subgroups within complications have distinct risks useful for ranking in the tier system.
Methods • INTERMACS data for all primary implants of CF devices implanted between 4/2012 and 3/2014 • DT and BTT included unless otherwise specified • Complications: • Multiple complications per time point • First and isolated complication • First infection of any number reported • OPTN/UNOS registry data for patients without MCS
Outcome • Death during VAD support • Censoring at transplantor recovery
Sample • 4725 primary CF VAD implants • 22,524 complications • 2975 1st and isolated complications • No AE report n=641 • Final cohort: n= 3616
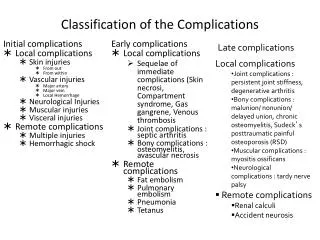
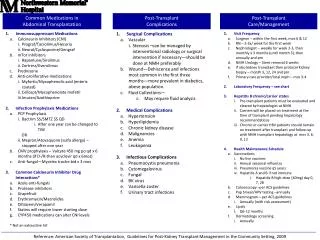
INTERMACS AEs Hemolysis Respiratory Failure Right Heart Failure Venous Thromboembolism Device Malfunction Wound Dehiscence Major Bleeding Arterial Non-CNS embolism Major Infection Other SAE Neurological Dysfunction Hepatic Dysfunction Cardiac Arrhythmias Hypertension Pericardial Fluid Collection Myocardial Infarction Psychiatric Episode Renal Dysfunction
Mortality following first AE reported Status 1A Status 1B
1st Infection AE N= 4632
Comparison to OPTN Status Status 1A Status 1B
Infection Definition OPTN INTERMACS Localized non-device Driveline or pump pocket Sepsis Internal pump component One of: • Symptoms along driveline with leukocytosis AND: • + blood culture • + site culture • Surgical debridement AND + site culture • + pump pocket culture • Bacteremia 4 wks s/p treatment Meyer D, et. al. American Journal of Transplantation 2015; 15: 44–54; http://www.uab.edu/medicine/intermacs/appendices-4-0/appendix-a-4-0
INTERMACS subgroups All p-values <0.01 vs. No infection AE
INTERMACS AEs & OPTN status Driveline vs. No inf. AE p=0.13 All other p-values <0.01 Status 1A Status 1B
Tier Proposals • MCS with arrhythmias, non-dischargeable VAD • MCS sepsis OR pump pocket/internal device infection OR localized infection, IABP • MCS driveline infection, thromboembolism, LVAD 30 days, dual inotropes • Inotrope w/o HD monitor, stable VAD Meyer D, et. al. American Journal of Transplantation 2015; 15: 44–54
Considerations • How should continued eligibility be weighted in priority decisions?
Changing device strategy Teuteberg J, et. al. J Am CollCardiol HF 2013
Considerations • How many subgroups should be identified and analyzed?
Stratified complications? Yes No Device malfunction Maybe • Infections • Right heart failure • Bleeding • Hemolysis • Ventricular arrhythmias • Thrombosis • Aortic regurg.
Conclusions Subgroups of patients within broad complication types may warrant further characterization and stratification by INTERMACS definitions
Susan Meyer • Frank Pagani • Kent Shively
Risk of first AE relative to Status 1A/B Status 1A Status 1B