Download
1 / 1
10 likes | 134 Views
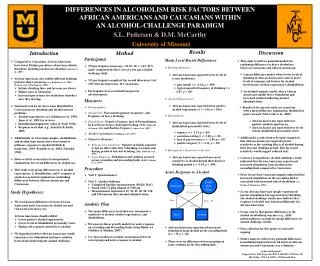
Perceived Mistreatment and Coping Strategies of African Americans and Caucasians with Cancer. Lauren Smith 1 , Thomas V. Merluzzi 1 , Errol J. Philip 2. 1 University of Notre Dame 2 Memorial Sloan Kettering Cancer Center. Background

E N D
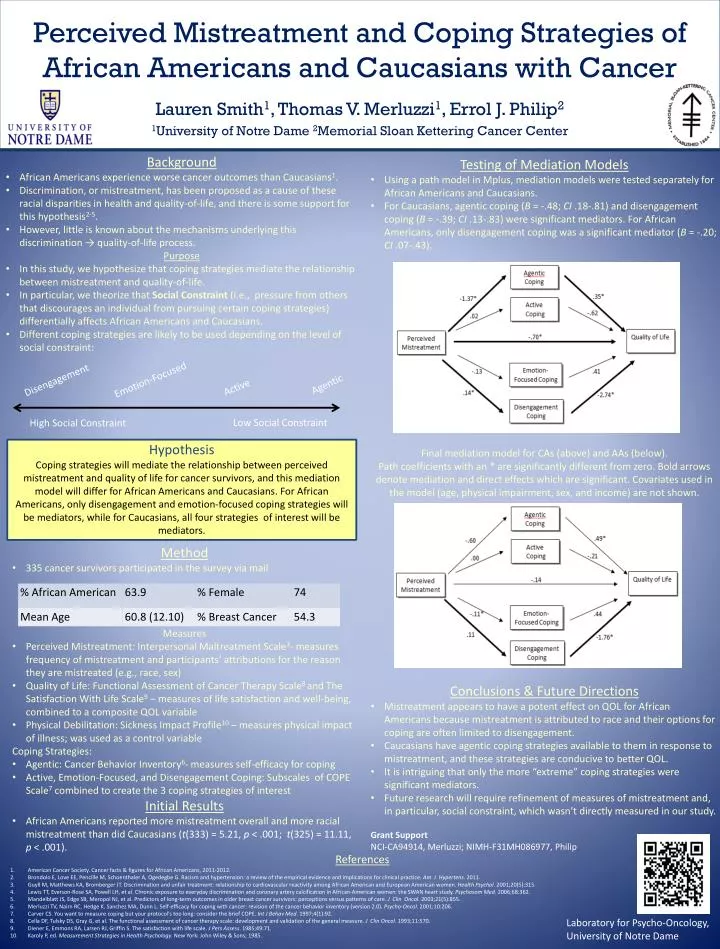
Perceived Mistreatment and Coping Strategies of African Americans and Caucasians with Cancer Lauren Smith1, Thomas V. Merluzzi1, Errol J. Philip2 1University of Notre Dame 2Memorial Sloan Kettering Cancer Center • Background • African Americans experience worse cancer outcomes than Caucasians1. • Discrimination, or mistreatment, has been proposed as a cause of these racial disparities in health and quality-of-life, and there is some support for this hypothesis2-5. • However, little is known about the mechanisms underlying this discrimination → quality-of-life process. • Purpose • In this study, we hypothesize that coping strategies mediate the relationship between mistreatment and quality-of-life. • In particular, we theorize that Social Constraint(i.e., pressure from others that discourages an individual from pursuing certain coping strategies) differentially affects African Americans and Caucasians. • Different coping strategies are likely to be used depending on the level of social constraint: • Testing of Mediation Models • Using a path model in Mplus, mediation models were tested separately for African Americans and Caucasians. • For Caucasians, agenticcoping (B = -.48; CI .18-.81) and disengagement coping (B = -.39; CI .13-.83) were significant mediators. For African Americans, only disengagement coping was a significant mediator (B = -.20; CI .07-.43). • Final mediation model for CAs (above) and AAs (below). • Path coefficients with an * are significantly different from zero. Bold arrows denote mediation and direct effects which are significant. Covariates used in the model (age, physical impairment, sex, and income) are not shown. • Conclusions & Future Directions • Mistreatment appears to have a potent effect on QOL for African Americans because mistreatment is attributed to race and their options for coping are often limited to disengagement. • Caucasians have agentic coping strategies available to them in response to mistreatment, and these strategies are conducive to better QOL. • It is intriguing that only the more “extreme” coping strategies were significant mediators. • Future research will require refinement of measures of mistreatment and, in particular, social constraint, which wasn’t directly measured in our study. • Grant Support • NCI-CA94914, Merluzzi; NIMH-F31MH086977, Philip Agentic Emotion-Focused Active Disengagement Low Social Constraint High Social Constraint Hypothesis Coping strategies will mediate the relationship between perceived mistreatment and quality of life for cancer survivors, and this mediation model will differ for African Americans and Caucasians. For African Americans, only disengagement and emotion-focused coping strategies will be mediators, while for Caucasians, all four strategies of interest will be mediators. • Method • 335 cancer survivors participated in the survey via mail • Measures • Perceived Mistreatment: Interpersonal Maltreatment Scale3- measures frequency of mistreatment and participants’ attributions for the reason they are mistreated (e.g., race, sex) • Quality of Life: Functional Assessment of Cancer Therapy Scale8 and The Satisfaction With Life Scale9 – measures of life satisfaction and well-being, combined to a composite QOL variable • Physical Debilitation: Sickness Impact Profile10 – measures physical impact of illness; was used as a control variable • Coping Strategies: • Agentic: Cancer Behavior Inventory6- measures self-efficacy for coping • Active, Emotion-Focused, and Disengagement Coping: Subscales of COPE Scale7 combined to create the 3 coping strategies of interest • Initial Results • African Americans reported more mistreatment overall and more racial mistreatment than did Caucasians (t(333) = 5.21, p < .001; t(325) = 11.11, p < .001). • References • American Cancer Society. Cancer facts & figures for African Americans, 2011-2012. • Brondolo E, Love EE, Pencille M, Schoenthaler A, Ogedegbe G. Racism and hypertension: a review of the empirical evidence and implications for clinical practice. Am J Hypertens. 2011. • Guyll M, Matthews KA, Bromberger JT. Discrimination and unfair treatment: relationship to cardiovascular reactivity among African American and European American women. Health Psychol. 2001;20(5):315. • Lewis TT, Everson-Rose SA, Powell LH, et al. Chronic exposure to everyday discrimination and coronary artery calcification in African-American women: the SWAN heart study. Psychosom Med. 2006;68:362. • MandelblattJS, Edge SB, Meropol NJ, et al. Predictors of long-term outcomes in older breast cancer survivors: perceptions versus patterns of care. J ClinOncol. 2003;21(5):855. • Merluzzi TV, Nairn RC, Hedge K, Sanchez MA, Dunn L. Self-efficacy for coping with cancer: revision of the cancer behavior inventory (version 2.0). Psycho-Oncol. 2001;10:206. • Carver CS. You want to measure coping but your protocol's too long: consider the brief COPE. Int J Behav Med. 1997;4(1):92. • CellaDF, Tulsky DS, Gray G, et al. The functional assessment of cancer therapy scale: development and validation of the general measure. J ClinOncol. 1993;11:570. • Diener E, Emmons RA, Larsen RJ, Griffin S. The satisfaction with life scale. J Pers Assess. 1985;49:71. • Karoly P, ed. Measurement Strategies in Health Psychology. New York: John Wiley & Sons; 1985. Laboratory for Psycho-Oncology, University of Notre Dame