Download
1 / 22
220 likes | 252 Views
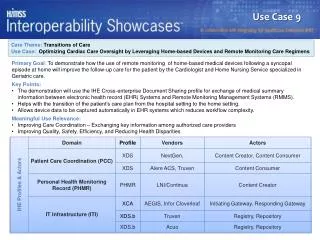
Understand challenges in care transitions, communication issues, discharge options, medication management, and patient perspectives. Real cases highlight complexities in the care continuum.

E N D
Care Transitions Manuel A. Eskildsen, MD Division of Geriatric Medicine and Gerontology Emory University School of Medicine
Objectives • Define why transitions between different settings of care may result in poor patient outcomes. • Explain how communication problems between health providers and patients result in poor care transitions. • Define the different discharge options for a patient leaving the hospital.
Why does this matter? Patients are sick when they go to the hospital Patients in hospitals have more chronic health problems They are usually not 100% well when they leave the hospital Many things can go wrong when they leave… And go somewhere else www.janga.biz
What is Transitional Care? • Coordination that occurs when patients transfer between settings of care. • Communication needs to occur between physicians between different levels of care. • Discharge sites: • Home • Assisted living • A nursing facility for rehabilitation • Another hospital (for example, acute rehab)
Poor transitions can lead to: • Readmission to the hospital • Medication errors • Poor communication and patient dissatisfaction • Poor continuity of care because of poor communication with primary physician
Why is it difficult for patients? • You may still not feel well when you leave the hospital • You may have multiple new medications, and different doses of the old ones • Many new appointments. For example, a pt. with hip fracture, could have to see: • Primary care doctor • Orthopedist • Therapists • Home health nurses
Your cases for today • Complex care transitions • Difficulties in communication • Difficulties with medications • Different perspectives: • Hospital MD • Patient/Family • Case Manager • Receiving MD
Case 1 • 81 year old woman with CHF • Admitted with shortness of breath, leg swelling • Similar hospital stay last month • Given increases in diuretic doses in the hospital • By the way, daughter having increasing problems caring for her
Case 1 • Daughter is concerned about taking her home • They decide on transfer to the Golden Years Assisted Living Facility • They meet with nurse for 20 minutes • Doctor waits for a week to dictate discharge summary
Medication lists for Case 1 • Aspirin 81 mg per day • Furosemide (diuretic) 40 mg per day • Atenolol (beta blocker blood pressure agent) 25 mg per day • Atorvastatin (cholesterol drug) 40 mg per day • Lisinopril (ACE inhibitor blood pressure agent) 20 mg per day • Aspirin 81 mg per day • Furosemide 40 mg twice a day • Metoprolol (beta blocker blood pressure agent) 25 mg twice a day • Simvastatin (cholesterol drug) 40 mg once a day • Enalapril (ACE inhibitor blood pressure drug) 20 mg twice a day
Case 1 • Returns to her doctor’s office with a bagful of medications • The primary care doctor could only obtain history from the family • Discharge Summary was not available
Points that you brought up: • Involvement of the doctor is important • Transitions are confusing for patients, and more so when caregivers are stressed • Incentive for the hosp. physician to “get people out” • Hospitalist wants to avoid readmission • Difficulty for PCP to keep up with all his patients who are in the hospital • Importance of the discharge summary for continuity
Assisted Living • Type of Senior Housing • For people with increasing care needs • They coordinate care • Help with meals, activities • Preserve a certain amount of independence • Preserves a sense of community
Home Health Services • Run by home health agencies • Supervised by a physician • For patients who are “homebound” • Include: • Nursing services (wound care, blood draws) • Physical therapy • Occupational Therapy
Case 2 • 88 year old man presented to EUH after a fall • X-ray shows a hip fracture • Had surgery – total hip replacement • Very complicated hospital course: confused, not able to ambulate much
Case 2 • Prior level of functioning: • Lived alone • Disheveled apartment • Repeated falls • Case manager and family agree that he is not ready to return home, and that he needs rehab at a Skilled Nursing Facility (SNF)
Case 2 • On day #8, the patient is discharged to a SNF for rehab • Still confused and weak • Receiving doctor gets a stack of papers and the medication list • Notes that the patient is still in pain • Patient and family are apprehensive – they don’t want to be in a “nursing home”
What you thought • What is a SNF? Why am I being “dumped” there? • Need for case manager to explain different options for discharge site • Agreement that home is not realistic option • Difficult role of the receiving physicians– dealing with patient expectations • Continuing focus on independence even after transfer to SNF
Skilled Nursing Facilities (SNF) • Can provide two different types of services • Residential care • Transitional care • For transitional care, patients come temporarily for: • Usually because they can’t receive needed services at home • For skilled services like rehabilitation • Physician care not as intense as in the hospital
SNF – Residential Care • For patients who cannot meet their care needs at home • Two “typical” patients: • The patient who is so immobilized that they need heavy care just to move from bed to toilet • Patient with Alzheimer’s dementia whose family can’t manage them at home
Better Care Transitions • Protocols in hospitals for discharge medications and communication • Discussion of “red flags” • Programs for nurse follow-up of hospital patients at home • Mandatory discharge summaries at time of discharge • More involvement of hospital physician in the discharge process