Download
1 / 45
450 likes | 619 Views
Diagnosis and Staging. JoAnne Zujewski, MD Head, Breast Cancer Therapeutics Clinical Investigations Branch Cancer Therapy Evaluation Program Division of Cancer Diagnostics and Treatment May 2011. NEJM, November 23, 2000. Early Detections reduces the risk of dying from breast cancer.

E N D
Diagnosis and Staging JoAnne Zujewski, MD Head, Breast Cancer Therapeutics Clinical Investigations Branch Cancer Therapy Evaluation Program Division of Cancer Diagnostics and Treatment May 2011
Early Detections reduces the risk of dying from breast cancer.
Cancer Diagnosis: Defining the Cancer • The first step in designing the treatment plan is carefully defining the cancer • Clinical examination • Radiology tests • Pathology tests • Blood tests
None Lump or mass Pain in breast Tenderness Thickening Firmness Nipple discharge Skin redness Asymmetry Enlargement Nipple retraction Dimpling Mass in axilla (armpit) Warmth Breast Cancer Signs and Symptoms
Defining the Cancer: Radiology • Radiologic imaging can help determine the location and spread of the cancer • Local extent • Regional lymph nodes • Distant spread (metastases)
Mammography Sensitivity in Younger Women • Screening mammograms miss up to 25% of breast cancers in women in their 40s, compared to 10% of cancers for older women
Breast MRI • Important new tool for imaging the breast • High sensitivity • Detection and characterization of otherwise-occult breast carcinoma
Breast Cancer Diagnosis • Any breast change or lump needs to be evaluated • Breast cancer needs to be diagnosed by biopsy • Fine needle aspiration • Core needle biopsy • Surgical biopsy
Mammotone & Minimally Invasive Breast Biopsy (MIBB) The Mammotone and MIBB are different from the core needle biopsy in that a needle is inserted once and multiple specimens are removed through contiguous sampling. Core needle biopsies require the needle to be inserted multiple times. Both the Mammotone and MIBB biopsy utilize a vacuum system. A probe is inserted and samples of tissue are collected in a chamber. Tissue samples are removed by action of a gentle vacuum.
Advantages of Needle Biopsies • Simple procedure – does not require surgery • Accurate • Quick – only takes a few minutes • Not painful • Inexpensive • Quick results
Disadvantages of Needle Biopsies • Entire lump is not removed • Open biopsy may be necessary For Fine Needle Only: • Specialist needed to read results • In situ cancer not distinguishable from invasive cancer
Image Guided Biopsy in Clinical Practice • Allows treatment planning • Better cosmesis • Can mark site with clip • Less costly • Needs specialized equipment • May still require confirmatory pathology in minority of cases
Breast Biopsy A core needle biopsy of the area is recommended Non-Surgical Surgical
Needle Biopsies • Fine Needle – A thin, hollow needle is used to remove a sample of tissue. The procedure is quick and can be done in a doctor’s office. • Core Needle – A larger needle is inserted through a small incision in the skin, and a small core of tissue is removed. This type of needle biopsy is done with the assistance of mammography or ultrasound imaging using stereotactic techniques with the aid of the computer, which calculates the precise location of the lump.
Incisional Biopsy • A surgical procedure where only a portion of a tumor is removed • Generally reserved for lumps that are larger • Performed under local anesthesia in a hospital or outpatient clinic
Excisional Biopsy • A surgical procedure that removes the entire suspected area plus some surrounding normal tissue. • Standard procedure for lumps that are smaller than an inch or so in diameter • Similar to a lumpectomy • Performed under local anesthetic or general anesthesia in a hospital or outpatient clinic
Advantages of Open Biopsies • Quick – takes only one hour • More accurate than a needle biopsy • Larger samples provide information for treatment plan Excisional Only: • Removes entire lump • May be the only surgical treatment needed
Disadvantages of Open Biopsies • Surgical procedure • Expensive • Side effects such as infection or blood collection under the skin Excisional Only: • Removing tissue can change the look and feel of the breast
Breast cancerSpread to lymph nodes Supraclavicular Subclavicular Distal (upper) axillary Central (middle) axillary Proximal (lower) axillary Mediastinal Internal mammary Interpectoral (Rotter’s)
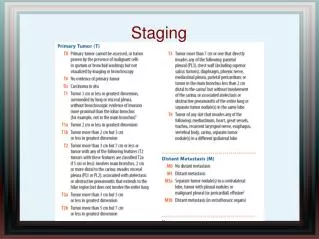
Breast Cancer: Stage I T1 N0 M0 T1a: T 0.5 cm T1b: 0.5 cm < T 1 cm T1c: 1 cm < T 2 cm T1 T 2 cm N0 = no regional lymph node metastasisM0 = no distant metastasis
Breast Cancer: Stage IIA } T0 T1 T2 N0 M0 N1 M0 No evidence of tumor T0 T2 2 cm < T < 5 cm N1 = metastasis to movable ipsilateral axillary lymph node(s)M0 = no distant metastasis
Breast Cancer: Stage IIB T2 N1 M0 T3 N0 M0 T3 T > 5 cm N1 = metastasis to movable ipsilateral axillary lymph node(s) (p) N1a, N1bM0 = no distant metastasis
T0 T1 T2 T3 N2 M0 Breast Cancer: Stage IIIA T3 N1 M0 Metastasis to ipsilateral axillary lymph node(s) N1 = movable N2 = fixed to one another or to other structures M0 = no distant metastasis
Breast Cancer: Stage IIIB Any T N3 M0 T4 any N M0 T4 Tumor of any size with direct extension to chest wall or skin T4d = inflammatory carcinoma N3 = metastasis to ipsilateral internal mammary lymph node(s) M0 = no distant metastasis
Breast Cancer: Stage IV Any T any N M1 M1 = distant metastasis (including metastases to cervical, or contralateral internal mammary lymph nodes)
Staging for Distant Disease: Breast Cancer FDG PET scan Bone Scan Patient A Patient B Multiple bone metastases Tumor in the breast, but not elsewhere The most common sites of distant disease in breast cancer are the bones, liver and lungs
80% 60% 5-Year Survival 40% 20% 0% 0 1 2 3 4 5 6-10 11-15 16-20 >20 Number of Positive Nodes BREAST CANCER5-year survival: Number of positive axillary lymph nodes Harris J, et al. Cancer: Principles & Practice of Oncology. 5th ed. 1997;1557-1616.
How effective is therapy for breast cancer? Relative 5 Year Survival (%) SEER, 1973-2003, DCP, NCI, 2009