Download
1 / 53
630 likes | 1.6k Views
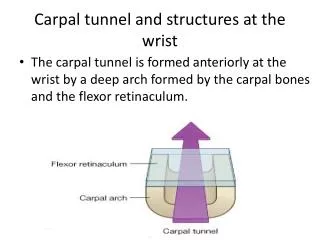
Wrist Biomechanics and Carpal Instability. Wrist Biomechanics. Anatomy Kinematics Force transmission. Anatomy. 8 bones Complex interlocking shapes Intrinsic and extrinsic ligaments. Wrist ligaments. Wrist ligaments. Volar stronger than dorsal

E N D
Wrist Biomechanicsand Carpal Instability MUN ORTHOPEDICS
Wrist Biomechanics • Anatomy • Kinematics • Force transmission MUN ORTHOPEDICS
Anatomy • 8 bones • Complex interlocking shapes • Intrinsic and extrinsic ligaments MUN ORTHOPEDICS
Wrist ligaments MUN ORTHOPEDICS
Wrist ligaments • Volar stronger than dorsal • Double V shape with weak area ; space of Poirier • Important interosseous ligaments are SLIL and LTIL • Dorsal ligaments tend to converge on triquetrum MUN ORTHOPEDICS
Kinematics • Three axes of motion • FEM 90 – 70 degrees • Flex/ext split between radiocarpal & midcarpal • RUD 20 – 50 degrees • PSM 90 – 90 degrees MUN ORTHOPEDICS
Axes of Motion MUN ORTHOPEDICS
Kinematics • Rows • Columns (Navarro) • Oval ring • Longitudinal columns (Weber) • “Link Joint” MUN ORTHOPEDICS
Link Joint MUN ORTHOPEDICS
Kinematics • Rows • Proximal and Distal with scaphoid as a bridge • Motion within and between rows • Columns • Central(flex/ext) lunate,capitate,hamate • Lateral (mobile) scaphoid,trapezoid,trapezium • Medial (rotation) triquetrum MUN ORTHOPEDICS
Kinematics • Center of rotation : head of capitate MUN ORTHOPEDICS
Kinematics • Radial deviation : scaphoid flexes proximal pole goes dorsal “pulling” lunate into palmar flexion • Ulnar deviation : scaphoid extends proximal pole goes volar pulling lunate into dorsiflexion MUN ORTHOPEDICS
Kinematics • Triquetrohamate helicoid joint • Ulnar deviation : “low” position distal and dorsiflexed pulling lunate into dorsiflexion • Radial deviation : “high”position proximal and palmar flexed pulling lunate into palmar flexion MUN ORTHOPEDICS
Force Transmission • Principal force transmission is through capitate lunate and proximal pole of scaphoid • 75% radius 25% ulna MUN ORTHOPEDICS
Classification of Carpal Instability • CID (dissociative) • DISI • VISI • CIND (non-dissociative) • Radiocarpal,Midcarpal,Ulnar transloc’n • CIC (complex) • Perilunate Dislocation MUN ORTHOPEDICS
Progressive periLunate Instability • Stage I – scapholunate instability • Stage II – capitate dislocation • Stage III – triquetral dislocation • Stage IV – lunate dislocation • Spectrum of injury MUN ORTHOPEDICS
PLI MUN ORTHOPEDICS
Mechanism of injury • Impact on thenar side of wrist causes hyperextension , ulnar deviation and intercarpal supination • Progressive damage around lunate • Bony or ligamentous MUN ORTHOPEDICS
Normal wrist MUN ORTHOPEDICS
Volar Intercalated SegmentInstability MUN ORTHOPEDICS
Dorsal Intercalated SegmentInstability MUN ORTHOPEDICS
Gilula lines MUN ORTHOPEDICS
Carpal Angles MUN ORTHOPEDICS
Carpal Height • L2/L1 = 0.54 • New ratio L2/capitate = 1.57 MUN ORTHOPEDICS
Scapholunate Instability • Most common form • Rarely diagnosed acutely • Local tenderness • Scaphoid shift(Watson) • Associated with other injuries eg distal radius MUN ORTHOPEDICS
Scapholunate Instability:Classification • Type 1 – dynamic • Neg Xray;+ve Watson:+ve cine • Type 2 – static • +ve plain films • Type 3 – degenerative • Type 4 – secondary • Kienbock’s ; SNAC MUN ORTHOPEDICS
Scapholunate Instability:Radiographs • Scapholunate gap >2mm • Foreshortened scaphoid • Cortical ring sign • Taliesnik,s “V” sign • Lack of parallelism? MUN ORTHOPEDICS
Scapholunate Instability MUN ORTHOPEDICS
DISI MUN ORTHOPEDICS
Scapholunate Instability MUN ORTHOPEDICS
Scapholunate Instability:Treatment • Acute (0-3 wks) : open repair vs arthroscopically-assisted PCP x 8wks • Chronic (>4 wks) : repair + reconstruction • STT • Blatt • SLC MUN ORTHOPEDICS
Scapholunate instability MUN ORTHOPEDICS
Acute repair SLIL MUN ORTHOPEDICS
Blatt Capsulodesis MUN ORTHOPEDICS
STT Fusion MUN ORTHOPEDICS
STT Arthrodesis MUN ORTHOPEDICS
Scapholunate Instability:Arthrosis • SLAC • PRC • Arthrodesis • RSL MUN ORTHOPEDICS
Triquetrolunate instabliity • Limited understanding of ulnar side • TL or TH ?? • Ulnar pain post injury • Click • +ve ballottement test • Beware ulnar impaction syndrome • Conservative Rx; rarely need limited fusion MUN ORTHOPEDICS
VISI MUN ORTHOPEDICS
Perilunate Dislocation • Perilunate & Lunate are same basic injury • Still missed in ER • Rx of choice : open reduction & repair of ligaments/bones • Dorsal and volar approach • Late: fusion or PRC MUN ORTHOPEDICS
Lesser and Greater arcs MUN ORTHOPEDICS
Perilunate Dislocation MUN ORTHOPEDICS
Perilunate repair MUN ORTHOPEDICS
Ulnar Translocation • Rare • Difficult to treat • Non-traumatic causes : RA,Madelung’s MUN ORTHOPEDICS
Ulnar Translocation MUN ORTHOPEDICS