Download
1 / 57
660 likes | 1.8k Views
DISORDERS OF THE UPPER AIRWAY. PN 132. Learning Objectives. Identify common disorders / diseases of the upper respiratory system Discuss etiology and pathophysiology associated with disorders / diseases of the upper airway

E N D
Learning Objectives • Identify common disorders / diseases of the upper respiratory system • Discuss etiology and pathophysiology associated with disorders / diseases of the upper airway • Identify cardinal signs and symptoms associated with disorders / diseases of the upper airway • Identify components used in the management of a client with an upper respiratory disorder or illness • Discuss assessment, diagnostic, nursing interventions and management, and patient education important to clients with upper respiratory disorders
Common Respiratory Infections • Acute Rhinitis • Acute Follicular Tonsillitis • Laryngitis • Pharyngitis • Sinusitis
Acute Rhinitis (Coryza) • Etiology and Pathophysiology • Also known as the “common cold” • Inflammation of mucous membranes in nose and sinuses • Usually caused by one or more viruses • Can be complicated by bacterial infection • Contaminate hands when coughing or sneezing • Spreads by touching things • Commonly spread by shaking hands with infected person • Signs and Symptoms • Evident within 24 to 48 hours after exposure • Increased sinus drainage • Postnasal drip • Throat irritation • Headache • Earache • Fever
Acute Rhinitis (Coryza) • Diagnostics and Labs • Throat and sputum cultures • Medical Treatment • No treatment available for Coryza • Treat symptoms • ASA, Tylenol to reduce fever • Cough suppressantfor non-productive cough • Expectorant for productive cough • Antibiotics if bacterial
Acute Follicular Tonsillitis • Etiology and Pathophysiology • Inflammation of the tonsils • Results from airborne or foodborne bacterial infection • Commonly streptococcus • Most common in school age children • Signs and Symptoms • Sore throat • Fever • Chills • General muscle aching • General malaise • Elevated WBCs • Increased throat secretions • Enlarged tonsils
Acute Follicular Tonsillitis • Diagnostics and Labs • Throat Cultures • CBC (to determine WBC count) • Medical Treatment • Antibiotics • Elective tonsillectomy and adenoidectomy (T&A) • Tonsils and adenoids are surgically excised • Usually for those who have recurrent attacks • Analgesics and antipyretics • Warm saline gargles
Laryngitis • Etiology and Pathophysiology • Often occurs secondary to another respiratory infection • Common disorder • Acute and/or chronic • Acute Laryngitis • Can cause respiratory distress in young children (small larynx) • Chronic • Usually associated with inflammation of laryngeal mucosa or edema in vocal cords • Accompanies viral or bacterial infections • Other Causes • Excessive use of the voice • Inhalation of irritating fumes
Laryngitis • Signs and Symptoms • Hoarseness • Complete voice loss • Throat feels scratchy and irritated • Patient may have persistent cough • Diagnostics and Labs • Laryngoscopy • Visualizes edema, drainage • Medical Management • Antibiotics (if bacterial) • Analgesics or antipyretics • Antitussives (to relieve cough) • Throat lozenges
Pharyngitis • Etiology and Pathophysiology • May be chronic or acute • Most common throat inflammation • Frequently accompanies the common cold • Usually viral • Can be caused by bacteria • Streptococci • Staphylococci • Contagious for 2 to 3 days after the onset of signs and symptoms • Signs and Symptoms • Dry cough • Tender tonsils • Enlarged cervical lymph glands • Throat looks edematous • Throat soreness • Severe pain to scratchy • Difficulty swallowing
Pharyngitis • Diagnostics and Labs • Rapid strep screen (to detect streptococci) • Two throat swabs obtained so culture can be performed if strep screen test is negative • Medical Management • Antibiotics • Analgesics and antipyretics • Throat rinses and gargles • Rest • Vaporizer
Sinusitis • Etiology and Pathophysiology • Acute or chronic • Involves any sinus area • Can be viral or bacterial • Often complication of pneumonia or nasal polyps • Begins as upper respiratory tract infection that leads to sinus infection • Signs and Symptoms • Complaints of constant/severe headache • Pain and tenderness in the affected sinus area • Purulent exudate
Sinusitis • Diagnostics and Labs • Sinus X-ray and/or CT scan • Trans-illumination • Shining bright light into the mouth with the lips closed around it • Infected areas of sinuses will look dark • Unaffected areas will trans-illuminate • Medical Treatment • Nasal windows • Surgical incisions that allow sinuses to drain • Medication • Antibiotics • Analgesics • Antihistamines • Vasoconstrictors (nasal sprays)
Epistaxis (Nose Bleed) Pathophysiology Congestion of the nasal membranes that leads to rupture of the capillaries Abundance of capillaries in the nasal passages Frequently caused by Injury Primary or secondary disorder Can be related to Menstrual flow Hypertension With treatment, prognosis is good
Epistaxis • Etiology • Dryness • Chronic infection • Trauma • Topical corticosteroid use • Nasal spray abuse • Street drug use (cocaine) • Disorder that results in decreased platelet count • Bleeding can be prolonged if using • Aspirin • NSAIDS
Epistaxis Clinical Manifestations Bright, red blood One or both nostrils Severe hemorrhage Up to 1 liter of blood loss / hour Can result in EXSANGUINATION (rare) Fatal blood loss
Epistaxis • Assessment • Subjective Assessment • Patient interview • Ask about: • Duration • Severity of bleeding • Precipitating factors • Objective Assessment • Assess presence of bleeding • Anterior / posterior to nasal passage • Blood pressure (severe drop may be indication of shock) • Temperature • Pulse • Respirations • Evidence of hypovolemic shock
Epistaxis • Medical Intervention • Nasal packing • Cotton saturated with epinephrine • Cautery • Burning the bleeding vessel • Use of silver nitrate stick (chemical) • Balloon Tamponade • Foley-like catheter inflated in the nose • Antibiotics • Reduce chance of infection
Epistaxis • Diagnostics and Labs • Blood Labs • (HCT, PT, INR, PTT) • Blood loss severity • Clotting abnormalities • Nasal Endoscopy • Identify source of bleeding
Epistaxis • Nursing Diagnoses • Ineffective tissue perfusion: R/T Blood Loss • Risk for Aspiration: R/T Bleeding
Epistaxis • Nursing Interventions • Keep patient quiet • Sitting position / leaning forward • Reclining with head and shoulders elevated • Apply direct pressure • 10 to 15 minutes • Pinch lower soft portion of the nose • Apply ice compresses to the nose • Have patient suck on ice • If bleeding continues • Insert a small gauze pad into the bleeding nostril • Apply direct pressure • Monitor vital signs • Monitor for s/s hypovolemic shock • Anxiety • Cool , clammy skin • Confusion • Decreased urine output • Weakness • Pale skin color • Rapid breathing • Moist skin / sweating • unconsciousness
Epistaxis • Patient Teaching • Don’t pick or scratch in or around nares • Don’t blow the nose vigorously • Avoid dryness to the nose • Use: • Vaporizer • Saline or nasal lubricants • Avoid Aspirin and NSAIDs • Sneeze with mouth open • Don’t insert foreign objects into the nose
Pathophysiology Deviated Septum and Nasal Polyps Deviated Septum • Nasal septum deviates from the midline • Partial nasal obstruction Nasal Polyps • Tissue growths on nasal tissues
Etiology Deviated Septum and Nasal Polyps Deviated Septum Nasal Polyps Congenital abnormality Injury Prolonged sinus inflammation Allergies
Deviated Septum and Nasal Polyps Clinical Manifestations • Blockage of nostrils / Nasal congestion • Frequent nose bleeds • Facial pain • Headache • Post nasal drip • Noisy breathing during sleep • (infants and children) • Dyspnea (struggling / strenuous respirations) • Harsh snoring sounds (Stertorous Respirations)
Deviated Septum / Nasal Polyps Assessment Subjective Ask about: Previous injuries / infections Allergies Sinus congestion Complaints of Dyspnea Post nasal drip Objective Identify condition and location Rate and character of respirations Note s/s of dyspnea
Deviated Septum / Nasal Polyps Diagnostics Visual Examination Sinus Radiographic Studies Shadowy sinuses = polyps present - Deviated Septum
Medical Management Deviated Septum / Nasal Polyps • Surgical Correction • Nasoseptoplasty(to align nasal septum) • Nasal Polypectomy • Surgical removal of polyps • Following surgery • Nasal packing (controls bleeding) • Nasal irrigation (saline) • Petroleum jelly to nares (prevent drying) • Medications • Corticosteroids (Prednisone) • Cause polyps to decrease/ disappear • Antihistamines • Reduce allergy signs/symptoms • Decreases congestion • Antibiotics • To prevent infection • Analgesics • Relieve headache
Nursing Diagnoses Deviated Septum / Nasal Polyps • Ineffective airway clearance • R/T nasal exudates • Risk for injury • R/T trauma to bleeding site associated with vigorous nose blowing
Deviated Septum / Nasal Polyps Nursing Interventions Maintain patent airway and prevent infection Monitor for s/s of infection Monitor for s/s hemorrhage Maintain patient comfort
Deviated Septum / Nasal Polyps Patient Teaching Avoid: vigorous nose blowing coughing holding your breath while bearing down (at least 2 days post-op) Notify Physician if bleeding infection occurs Use nasal sprays and drops sparingly Facial edema and ecchymosis may appear post-op
Antigen-Antibody Allergic Rhinitis and Allergic Conjunctivitis HAY FEVER
Pathophysiology Hay Fever • Atopic allergic condition • Affects • Nasal membranes • Nasopharynx • Conjunctiva • Ciliary action slows • Mucosal gland secretion increases • Leukocyte infiltration occurs • Increased capillary permeability and vasodilation • Local tissue edema results
Hay Fever • Etiology • Antigen / Antibody Reaction • Inhalation or contact with allergens • Common allergens • Tree, Grass, Weed Pollen • Mold spores • Fungi • House dust • Mites • Animal dander • Foods • Drugs • Insect bites and stings
Hay Fever Clinical Manifestations and Assessment Photophobia Edema Blurred vision / watery eyes Pruritus Excessive tear production Cough / Sneezing Epistaxis Headache Congestion Excessive nasal secretions (rhinitis) Otitis media complaints of: Ear fullness and popping Decreased hearing • Chronic S/S • Headache • Severe nasal congestion • Post nasal drip • Cough • If untreated secondary infections may occur • Otitis media • Bronchitis • Sinusitis • pneumonia
Hay Fever • Diagnostics • Physical exam of eyes and ears • Skin Testing • RAST test (blood test • Measures allergy antibody produced when mixed with allergens
Hay Fever • Medical Management • Relieve symptoms • Avoid allergen • Antihistamines • Topical or Nasal Corticosteroids • Leukotriene Receptor Antagonists • Decongestants • Lodoxamide (conjunctivitis) • Analgesics (headache) • Hot Packs
Hay Fever Nursing Interventions • Self-limiting illness • Focus on: • Health promotion and self-care teaching • Ways to avoid allergens • Symptom control • Medication action and usage
Upper Airway Obstruction Etiology and Pathophysiology • Recent respiratory event • Trauma to the airway or to the surrounding tissues • Laryngeal spasm • Laryngeal edema • Common items that obstruct the upper airway are: • Choking on food • Dentures • Aspiration of vomitus or secretions • The tongue (the most common in an unconscious person)
Upper Airway Obstruction Clinical Manifestations Main Signs Stertorous or Stridor Respirations Altered respiratory rate and character Apneic periods
Upper Airway Obstruction Assessment Subjective Limited Difficult time with breathing Difficulty speaking Objective Signs of hypoxia Disorientation, fatigue, anxiety Cyanosis of the skin, lips, and nail beds Snoring, wheezing, or stridorous respirations Bradycardia Shallow, slow respirations (bradypnea)
Upper Airway Obstruction Diagnostics Medical emergency No diagnostic tests Prompt, accurate assessment and treatment
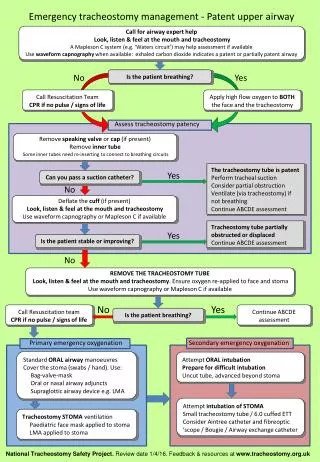
Upper Airway Obstruction Medical Management Abdominal Thrusts To remove obstruction Maintain patent airway Artificial Airway Endotracheal Pharyngeal Tracheal Emergency Tracheostomy (Video) • http://www.youtube.com/watch?v=d_5eKkwnIRs