Download
1 / 1
10 likes | 106 Views
Characteristics of Patients Using Extreme Opioid Dosages in the Treatment of Chronic Low Back Pain. Shannon Essler, 1 Sandra Burge, Ph.D., 2 Terrell Benold, M.D. 3 1 Southwestern University 2 University of Texas Health Science Center at San Antonio 3 Austin Family Medicine Residency Program.

E N D
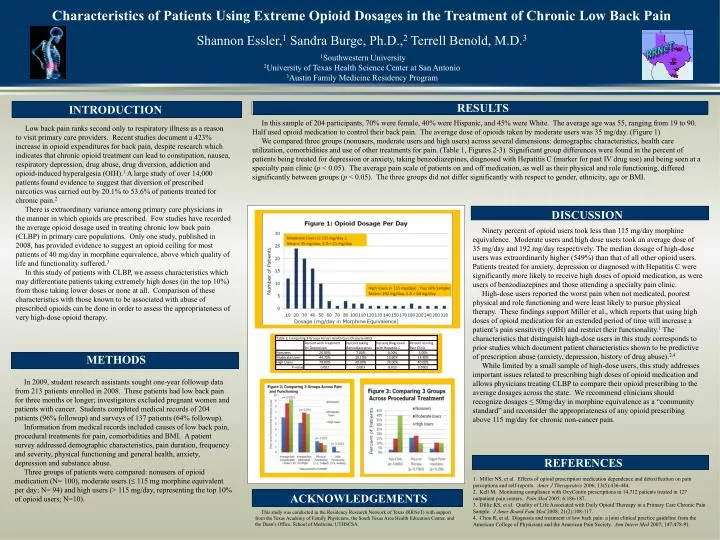
Characteristics of Patients Using Extreme Opioid Dosages in the Treatment of Chronic Low Back Pain Shannon Essler,1 Sandra Burge, Ph.D.,2 Terrell Benold, M.D.3 1Southwestern University 2University of Texas Health Science Center at San Antonio 3Austin Family Medicine Residency Program RRNeT RESULTS INTRODUCTION In this sample of 204 participants, 70% were female, 40% were Hispanic, and 45% were White. The average age was 55, ranging from 19 to 90. Half used opioid medication to control their back pain. The average dose of opioids taken by moderate users was 35 mg/day. (Figure 1) We compared three groups (nonusers, moderate users and high users) across several dimensions: demographic characteristics, health care utilization, comorbidities and use of other treatments for pain. (Table 1, Figures 2-3) Significant group differences were found in the percent of patients being treated for depression or anxiety, taking benzodiazepines, diagnosed with Hepatitis C (marker for past IV drug use) and being seen at a specialty pain clinic (p < 0.05). The average pain scale of patients on and off medication, as well as their physical and role functioning, differed significantly between groups (p < 0.05). The three groups did not differ significantly with respect to gender, ethnicity, age or BMI. Low back pain ranks second only to respiratory illness as a reason to visit primary care providers. Recent studies document a 423% increase in opioid expenditures for back pain, despite research which indicates that chronic opioid treatment can lead to constipation, nausea, respiratory depression, drug abuse, drug diversion, addiction and opioid-induced hyperalgesia (OIH).1 A large study of over 14,000 patients found evidence to suggest that diversion of prescribed narcotics was carried out by 20.1% to 53.6% of patients treated for chronic pain.2 There is extraordinary variance among primary care physicians in the manner in which opioids are prescribed. Few studies have recorded the average opioid dosage used in treating chronic low back pain (CLBP) in primary care populations. Only one study, published in 2008, has provided evidence to suggest an opioid ceiling for most patients of 40 mg/day in morphine equivalence, above which quality of life and functionality suffered.3 In this study of patients with CLBP, we assess characteristics which may differentiate patients taking extremely high doses (in the top 10%) from those taking lower doses or none at all. Comparison of these characteristics with those known to be associated with abuse of prescribed opioids can be done in order to assess the appropriateness of very high-dose opioid therapy. DISCUSSION Ninety percent of opioid users took less than 115 mg/day morphine equivalence. Moderate users and high dose users took an average dose of 35 mg/day and 192 mg/day respectively. The median dosage of high-dose users was extraordinarily higher (549%) than that of all other opioid users. Patients treated for anxiety, depression or diagnosed with Hepatitis C were significantly more likely to receive high doses of opioid medication, as were users of benzodiazepines and those attending a specialty pain clinic. High-dose users reported the worst pain when not medicated, poorest physical and role functioning and were least likely to pursue physical therapy. These findings support Miller et al., which reports that using high doses of opioid medication for an extended period of time will increase a patient’s pain sensitivity (OIH) and restrict their functionality.1 The characteristics that distinguish high-dose users in this study corresponds to prior studies which document patient characteristics shown to be predictive of prescription abuse (anxiety, depression, history of drug abuse).2,4 While limited by a small sample of high-dose users, this study addresses important issues related to prescribing high doses of opioid medication and allows physicians treating CLBP to compare their opioid prescribing to the average dosages across the state. We recommendclinicians should recognize dosages ≤ 50mg/day in morphine equivalence as a “community standard” and reconsider the appropriateness of any opioid prescribing above 115 mg/day for chronic non-cancer pain. METHODS In 2009, student research assistants sought one-year followup data from 213 patients enrolled in 2008. These patients had low back pain for three months or longer; investigators excluded pregnant women and patients with cancer. Students completed medical records of 204 patients (96% followup) and surveys of 137 patients (64% followup). Information from medical records included causes of low back pain, procedural treatments for pain, comorbidities and BMI. A patient survey addressed demographic characteristics, pain duration, frequency and severity, physical functioning and general health, anxiety, depression and substance abuse. Three groups of patients were compared: nonusers of opioid medication (N= 100), moderate users (≤ 115 mg morphine equivalent per day; N= 94) and high users (> 115 mg/day, representing the top 10% of opioid users; N=10). REFERENCES 1. Miller NS, et al. Effects of opioid prescription medication dependence and detoxification on pain perceptions and self-reports. Amer J Therapeutics 2006; 13(5):436-444. 2. Kell M. Monitoring compliance with OxyContin prescriptions in 14,712 patients treated in 127 outpatient pain centers. Pain Med 2005; 6:186-187. 3. Dillie KS, et al. Quality of Life Associated with Daily Opioid Thereapy in a Primary Care Chronic Pain Sample. J Amer Board Fam Med 2008; 21(2):108-117. 4. Chou R, et al. Diagnosis and treatment of low back pain: a joint clinical practice guideline from the American College of Physicians and the American Pain Society. Ann Intern Med 2007; 147:478-91. ACKNOWLEDGEMENTS This study was conducted in the Residency Research Network of Texas (RRNeT) with support from the Texas Academy of Family Physicians, the South Texas Area Health Education Center, and the Dean’s Office, School of Medicine, UTHSCSA.