Download
1 / 12
120 likes | 134 Views
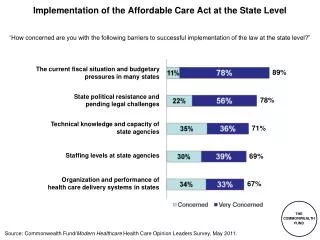
This presentation discusses the key influences affecting state-level implementation of the H1N1 vaccination campaign, including varying goals, relationships with key agencies, public health capacity, information infrastructure, and existing relationships with immunization providers. Lessons learned emphasize the importance of flexibility, building new relationships, and improving information systems for future vaccination efforts.

E N D
Tracking State-Level Implementation of H1N1 Vaccination Grantees Sarah Clark Child Health Evaluation and Research Unit (CHEAR) University of Michigan National Immunization Conference April 21, 2010
Background • H1N1 vaccine implementation was characterized by: • Federal guidance and structure • Flexible implementation at the program level • No existing mechanism to track implementation across states
Background • UM team collected situational awareness data on H1N1 vaccine implementation • September 2009 – February 2010 • Collaborative approach • Short-term feedback • Lessons learned based on experiences
Purpose • To describe some of the key influences on state implementation of H1N1 vaccination
Key Influences • States had varying goals for their H1N1 vaccine campaigns: • Make vaccine available to whoever wants it. • Vaccinate as many people as possible. • Vaccinate high-risk individuals first. • Goals established the perspective for key decisions
Key Influences • State immunization officials had varying relationships with other key agencies prior to H1N1: • Preparedness • Epidemiology • Education • Medical licensure
Key Influences • States have varying public health capacity: • Almost no public health departments • City/county/regional health departments that are agents of the state • City/county/regional health departments that are autonomous • Range of LPH: 1 to 350 • Variety of service delivery across LPH
Key Influences • States began the campaign with variable information infrastructure: • Immunization information systems • Databases of providers • Communication systems • States had variable IT support • New mechanisms needed for registration, allocation, doses administered reporting
Key Influences • States were highly variable in their existing relationships with other immunization providers and settings: • Hospitals • Adult immunization providers • Pharmacies and community vaccinators • Schools
Lessons Learned • Flexibility in implementation of H1N1 vaccination was essential to • accommodate existing state differences • allow for different choices • States should build on their H1N1 efforts • New relationships with providers and other state agencies • Information systems
Acknowledgments • University of Michigan team: Anne Cowan, Brian Macilvain, Gary Freed • AIM: Claire Hannan, Katelyn Wells • Immunization program officials