Download
1 / 21
210 likes | 352 Views
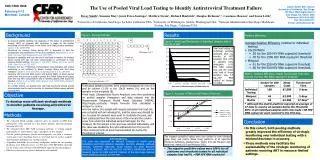
Outcomes in ART treatment programmes with and without access to routine viral load monitoring Olivia Keiser on behalf of IeDEA Southern Africa okeiser@ispm.unibe.ch. Background. Debate on place of routine viral load monitoring in scale-up programmes

E N D
Outcomes in ART treatment programmes with and without access to routine viral load monitoring Olivia Keiser on behalf of IeDEA Southern Africa okeiser@ispm.unibe.ch
Background • Debate on place of routine viral load monitoring in scale-up programmes • South Africa: routine VL monitoring part of national programme Malawi and Zambia: no routine viral load monitoring 2
Selection of patients/ programmes • Treatment naïve patients > 15 years, NNRTI-based ART regimen. All sites participate in IeDEA Southern Africasee: www.iedea-sa.org 3
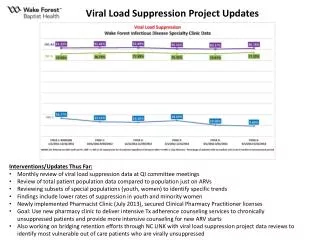
Mortality 0.10 No viral load monitoring(Malawi and Zambia) Routine viral load monitoring(South Africa) Cumulative mortality 0.05 0.00 0 1 2 3 Years since HAART start
Sites with and without (reference) VL monitoring Competing risk regression with loss to follow-up and start of second-line therapy as competing events *Adjusted for age, sex, CD4 cell count and clinical stage of disease 7
Sites with and without (reference) VL monitoring • Sites with < 15% loss to follow-up 2 years after ART start Competing risk regression *Adjusted for age, sex, CD4 cell count and clinical stage of disease 9
Expected non-HIV-related death rate per 100 pyrs * Based on South African rates 11
4) Delayed/missed detection of treatment failure and switching in non-VL sites? 12
Multistate model Treatment failure - virologic (viral load sites) - immunologic (non viral load sites) Six months after ART start Switch Death Loss to follow-up Putter et al., Stat Medicine 2007
1 0.75 Proportion of patients 0.5 0.25 0 From 6 months after ART start Non VL sites VL sites 0 200 400 600 800 0 200 400 600 800 Time (days) Time (days) Remaining on first-line ART Death Second-line therapy Loss to follow-up CD4 criteria for switching
1 0.75 Proportion of patients 0.5 0.25 0 From failure Non VL sites VL sites 0 200 400 600 800 0 200 400 600 800 Time (days) Time (days) Death Second-line therapy Loss to follow-up CD4 criteria for switching
1 0.75 Proportion of patients 0.5 0.25 0 From switch Non VL sites VL sites 0 200 400 600 0 200 400 600 800 800 Time (days) Time (days) Death Second-line therapy Loss to follow-up
1 0.75 Proportion of patients 0.5 0.25 0 0 200 400 600 800 From switch VL sites (linkage with death registry) Non VL sites 0 200 400 600 800 Time (days) Time (days) Death Second-line therapy Loss to follow-up
Conclusions • Mortality rate higher in sites without routine viral load monitoring • Difference probably not explained by differences in- Patient characteristics- Loss to follow-up- Background mortality • Alternative explanations: • Delayed/missed switching- Diagnostic and treatment capacities (for OIs), other differences in patient management 18
Diagnostic capacities Not generally available or off site yes no 19
Limitations • Few sites and countries included • Mortality in patients lost to follow-up unknown in many sites • Linkage with death registry only possible for patients with South African ID number available • Estimates of HIV-free mortality might be inaccurate This is an observational study - Ideally one would need a randomized trial 20
Acknowledgement University of Bern: Matthias Egger, Thomas Gsponer, Janne Estill, Gilles Wandeler, Franziska Schöni-Affolter, Martin Brinkhof, Fritz Käser, Claire Graber Data centerCape Town: Andrew Boulle, Morna Cornell, Leigh Johnson,Nicola Maxwell Site investigators: Benjamin Chi, Matt Fox, Mhairi Maskew, Catherine Orrell, Hans Prozesky, Ralf Weigel, Andrew Westfall 21