Download

1 / 31
310 likes | 545 Views
Good Morning! Welcome Applicants!. November 3, 2011. Normal Audiogram. Patient’s Audiogram. Classification. *Conductive → involving any cause that in some way limits the amount of external sound that gains access to the inner ear (usually temporary) More common in children

E N D
Good Morning! Welcome Applicants! November 3, 2011
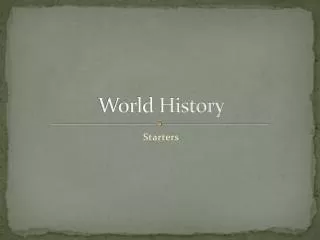
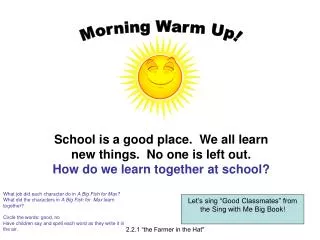
Normal Audiogram Patient’s Audiogram
Classification • *Conductive→ involving any cause that in some way limits the amount of external sound that gains access to the inner ear (usually temporary) • More common in children • Sensorineural→ involving the inner ear, cochlea, or the auditory nerve (more likely permanent) • Mixed→ which is a combination of conductive and sensorineural hearing loss. • Central→ involving higher brain centers.
Introduction • Hearing loss in the first years of life can cause delays in speech, language, and cognitive development • 1 to 6 per 1,000 newborns and 2 per 1,000 young children • With early intervention, hearing-impaired can reach same skill level of hearing peers
Question • 3-day-old infant failed otoacoustic emission testing (OAE). Prenatal and family histories are negative. Physical exam is normal. • The next most appropriate step is: • A. Confirm the hearing loss with an auditory brainstem response test • B. Perform renal ultrasound • C. Refer to audiology at 1 year of age • D. Repeat OAE in 6 months • E. Treat with oral abx for possible middle ear effusion
Screening • AAP recommends congenital hearing loss be detected by 1 month, diagnosed by 3 months, and intervention started by 6 months • Every state has universal newborn hearing screening • Otoacoustic emission testing (OAE) – detects evoked sound from the cochlea in response to clicks and tones • Auditory brainstem response (ABR) – measures the electroencephalographic waveform response from the vestibulocochlear nerve • Used to confirm abnormal OAE • All children ages 4 years and older should be screened regularly for hearing loss
Acquired Hearing Loss • History • Onset • Drainage • Tinnitus, vertigo, disequilibrium • Kidney or cardiac disease • Congenital infection, recurrent OM, meningitis • Trauma – noise exposure • Prematurity, hyperbilirubinemia • Family hx of hearing problems
Acquired Hearing Loss • Physical exam • Good head and neck exam • Ear exam • Pneumatic otoscopyis performed with positive and negative pressure to evaluate mobility of the tympanic membrane • Diminished or absent tympanic membrane mobility can be caused by fluid, mass in the middle ear cavity, perforation, pressure equalization tube, or sclerosis of the tympanic membrane. • Increased mobility of the tympanic membrane can indicate ossicular chain disruption.
Question • Which of the following statements regarding hearing loss in infants and children is TRUE? • A. Chidren with external ear anomalies have sensorineural hearing loss more than conductive hearing loss • B. Cholesteatoma is the most common cause of conductive hearing loss • C. Language delay does not occur unless hearing loss is severe or profound • D. Newborn hearing screens should be performed only on premature infants or those with family hx • E. Parental concern for language delay is sufficient cause for auditory testing
Office Hearing Tests • 256 Hz and 512 Hz tuning forks • Hearing loss at 256 Hz is equivalent to approximately 10 to 15 decibels (dB), and hearing loss at 512 Hz is equivalent to 20 to 30 dB
Office Hearing Tests • Pure tone audiometry • Softest decibel threshold at which the child can hear a sound 50 percent of the time for each tested frequency • Normal hearing threshold is between 0 to 20 dB • Accurate results are dependent upon cooperation from the child • Any threshold >20 dB suggests a hearing loss (conductive, sensorineural, or mixed).
Office Hearing Tests • OAE • Tympanometry • Valuable in conjunction with pneumatic otoscopy • *Flat tympanograms (type B tympanograms) and/or abnormal OAE testing may indicate conductive hearing loss, usually due to middle ear effusion
Referral • Any abnormal hearing screenings in the office should be followed by formal audiology
Etiologies of Acquired Conductive Hearing Loss • *Otitis media with effusion • Fluid filling the middle ear space prevents the tympanic membrane from vibrating adequately • Persistence of asymptomatic effusion following an episode of acute otitis media: • 40% at 1 month • 20% at 2 months • 10% at 3 months • These pts. may benefit from tympanostomy tubes
Etiologies of Acquired Conductive Hearing Loss • TM Perforation • Foreign Body
Etiologies of Acquired Hearing Loss • Cholesteatoma • Benign growth of stratified, squamous epithelium filled with desquamated cells and keratin • Erodes ossicular chain • Results from poor eustachian tube function
Question • A newborn who failed hearing screen, also has microcephaly, enlarged liver, and weight at 5th percentile. Pregnancy was uneventful, with normal prenatal labs, and there is no family history of hearing impairment. • Most likely cause of hearing impairment is: • A. Alport syndrome • B. Congenital CMV • C. Middle ear effusion • D. Prenatal measles exposure • E. Waardenburg syndrome
Etiologies of Hereditary Sensorineural Hearing Loss • Usher syndrome • Pendred syndrome • Waardenburg syndrome → • *Alport syndrome • Glomerular disease, ocular abnormalites, SNHL (progressive), family hx of hematuria, renal failure and deafness • Mitochondrial disorders
Etiologies of Acquired Sensorineural Hearing Loss • Bacterial meningitis • *Most common cause of acquired deafness in childhood • 2.5 to 18% • Occurs early in the course (within first 48 hours) • *Prompt and complete hearing evalutaion initially and regular follow-up
Etiologies of Acquired Sensorineural Hearing Loss • Noise exposure (acoustic trauma) • *High frequency hearing loss • Constant exposure to loud noises (personal listening devices, power tools, firearms) greater than 85 dB • Or sudden noise (firecracker) greater than 140 dB • 12.5% of kids (age 6 to 19) have hearing loss in one or both ears
Etiologies of Acquired Sensorineural Hearing Loss • Trauma • Temporal bone fracture • Bleeding from ear or hemotympanum
Treatment • Multidisiplinary approach • Audiology • ENT • Speech • Genetics • Optho referral • Patients rely on sight for communication and learning • Treatment based on etiology • Hearing aids • Cochlear implant
Noon conference Toddler Behavior, Dr. Nass