Download
1 / 46
881 likes | 2.72k Views
Onychomycosis. Hai Ho, M.D. Diagnosis?. Pitting Nail involvement – 10-50% Usually along with skin lesions, but could be alone Could occur in eczema, fungal infection, and alopecia areta. Psoriasis. Diagnosis?. Pitting. Onycholysis

E N D
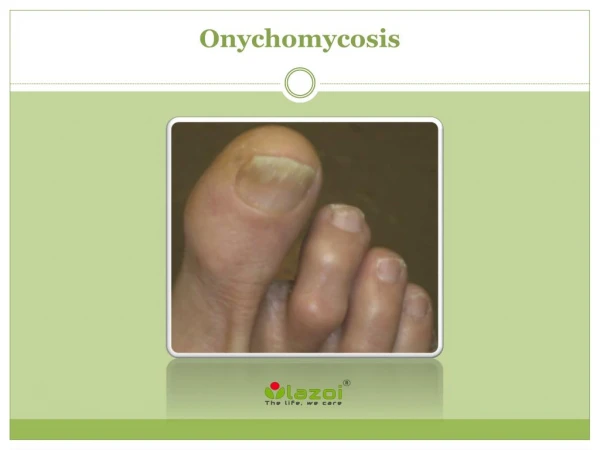
Onychomycosis Hai Ho, M.D.
Diagnosis? • Pitting • Nail involvement – 10-50% • Usually along with skin lesions, but could be alone • Could occur in eczema, fungal infection, and alopecia areta Psoriasis
Diagnosis? Pitting Onycholysis Yellow psoriatic debris under the nail causing nail separation Psoriasis
Diagnosis? Nail matrix involvement leading to nail deformity Psoriasis
Diagnosis? Onycholysis • Painless separation of the nail from the nail bed • Causes: trauma (long nail in women), hyperthyroidism, prolonged immersion, psoriasis
Diagnosis? Traumatic onycholysis
Onycholysis • May have secondary candida infection • Treatment • Avoid long nail • Tinture containing miconazole under nail • Fluconazole for resistant case
Diagnosis? Nail hypertrophy • Cause: tight-fitted shoes or chronic trauma • Treatment: filing or removing the nail with phenol
Diagnosis? Leukonychia punctata • Cause by cuticle manipulation or other mild trauma
Diagnosis? Leukonychia
Diagnosis? Distal splitting nail • Analogous to peeling of dry skin • Affected 20% of adults • Associated with water immersion and use of polish remover • Treatment • Moisturizer • B-complex vitamin biotin (2.5mg/day) for brittle nail
Diagnosis? Pincer nail • Due to ?tight shoes • Treatment • Nail removal • Reconstruction of nail unit
Diagnosis? Habit-tic onycholysis
Diagnosis? Median dystrophy
Moral of the story • Cannot diagnose onychomycosis by visualization alone • >50% of fungal-looking nail do not have fungal infection
Common organisms in onychomycosis? • Dermatophytes • Trichophytumrubum • Trichophytummentagrophytes • Contaminants or nonpathogens • Aspergillus, Cephalosporium, Fusarium, and Scopulariopsis
Distal subungual onychomycosis • Most common • Fungi invade the hyponychium and grow in the substance of nail plate, causing it to crumble • Hyperkeratotic debris causes nail to separate from the bed
Distal subungual onychomycosis Linear channel • Infection advance proximally • Characteristic feature of fungal infection
White superficial onychomycosis Commonly Trichophyton mentagrophytes Nail - white, soft, powdery
White superficial onychomycosis • Nail • not thickened • not separated from the nail bed
Proximal subungual onychomycosis • Commonly Trichophyton Rubrum • Invade the substance of nail plate, not the surface • Hyperkeratotic debris causes the nail plate to separate from the nail bed
Proximal subungual onychomycosis is associated with what disease? HIV
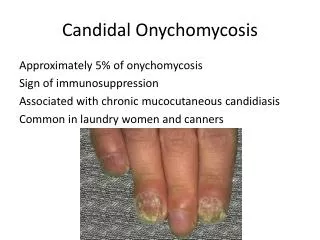
Candida onychomycosis • Almost exclusively in chronic mucocutaneous candidiasis • Generally infect all fingernails • Linear yellow or brown streaks grow and advance proximally
Candida onychomycosis Yellow areas with hyperkeratosis
Laboratory tests? • KOH – improve detection with fluorochrome which binds with chitin in fungal cell wall and fluoresces • Culture – gold standard • Histological examination by periodic acid-Schiff (PAS) staining – equal to culture
Obtaining specimen Clip the nail for PAS & culture Subungal debris for KOH & culture Fungi reside in the nail plate and cornified cells in the nail bed Hyphae in the nail plate may not be viable, so obtain specimen from nail bed for culture
KOH examination Hard nail plate and debris could be softened overnight with KOH Artifacts – lipid droplet between cells; eliminated by heat which separates cells
Culture • Sabouraud's with antibiotics • Antibiotics suppress bacterial contaminants • Medium turn from yellow to red in 7-14 days – alkaline released by dermatophytes turn phenol (pH indicator) red • ID the organism
PAS staining • In the presence of periodic acid, hydroxyl group of polysaccharide in fungal cell wall oxidized to aldehyde • Schiff reacts with aldehyde to stain fungal elements pinkish-red • False-negative – sampling error
Options • Systemic – terbinafine, itraconazole, fluconazole • Topical • Mechanical
Oral medications Terbinafine is more effective than itraconazole and fluconazole
Terbinafine vs. intermittent itraconazole Cure rate at 72 weeks Crawford F, et al. Arch Dermatol 2002; 138:811
Terbinafine vs. fluconazole Cure rate at 60 weeks Havu V, et al. Br J Dermatol 2000; 142(1):97.
Ineffective oral regimen • Intermittent terbinafine • Greseofulvin
Adverse effect of terbinafine? • Cholestatic hepatitis and blood dyscrasias • LFT and CBC prior to and at 6 weeks during treatment
Adverse effect of itraconazole? • Hepatitis for continuous but not intermittent regimen • LFT prior and at 6 weeks during treatment for continuous, not pulse, regimen
Drug interactions with itraconazole • Cytochrome P450 system • Arrhythmia with quinidine and primozile • Rhabdomyolysis with HMG-CoA reductase inhibitors, such as atorvastatin • Sedation and apnea with benzodiazepines • Decrease absorption with high gastric pH • Avoid H2-blocker and PPI • Take with food
Fluconazole • Not FDA approval for onychomycosis • First line for candida but could use for dermatophytes • Check LFT
Prevent recurrence • Prevent tinea pedis – powder to feet, protect feet in communal shower, change socks • Avoid trauma by tight shoes • Ciclopirox nail lacquer 8% (PENLAC) 2 to 3 times a week
Ciclopirox nail lacquer 8% (PENLAC) • Cure rate at 48 weeks – 29% • Apply to affected nail and 5 mm of surround skin daily • Remove PENLAC with alcohol weekly • Remove infected nail frequently
Mechanical removal • Surgery • Nonsurgical avulsion of dystrophic nail, not normal one
Nonsurgical avulsion • Apply 40% urea gel (Carmol-40 gel, Vanamide cream) with occlusive dressing • Remove the entire nail or cut the affected portion, followed by curetting to normal nail in 7-10 days